



Overview
Source: Joseph Donroe, MD, Internal Medicine and Pediatrics, Yale School of Medicine, New Haven, CT
While its usefulness in cancer screening is debated, the male rectal examination remains an important part of the physical exam. The exam is indicated in selected patients with lower urinary tract symptoms, urinary and/or fecal incontinence or retention, back pain, anorectal symptoms, abdominal complaints, trauma patients, unexplained anemia, weight loss, or bone pain. There are no absolute contraindications to the rectal exam; however, relative contraindications include patient unwillingness to undergo the exam, severe rectal pain, recent anorectal surgery or trauma, and neutropenia.
When performing the rectal exam, the examiner should conceptualize the relevant anatomy. The external anal sphincter is the most distal part of the anal canal, which extends three to four centimeters before transitioning into the rectum. The prostate gland lies anterior to the rectum, just beyond the anal canal. The posterior surface of the prostate, including its apex, base, lateral lobes, and median sulcus, can be palpated through the rectal wall (Figure 1). The normal consistency of the prostate is similar to the thenar eminence when the hand is in a tight fist. The thumb knuckle is representative of what a hard nodule may feel like. The normal size of the prostate increases with age and is approximately 4.0 cm by 3.5 cm, or 20-30 g, in a young man.
The steps of the male rectal exam, including preparation, positioning, neurologic assessment, external inspection and palpation, examination of the prostate and rectum, and evaluation of the stool, are detailed in this video.
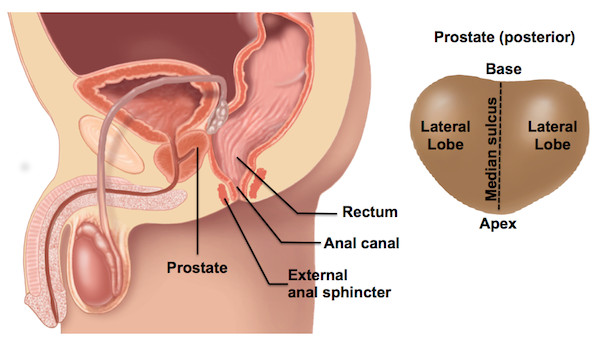
Figure 1. Male rectal anatomy (left) and regions of prostate gland posterior surface (right).
Procedure
1. Preparation
- Prepare the Patient
- Inform the patient of the exam about to be performed and the reason for it. Recognize that some men may feel uncomfortable at the idea of having the exam performed. If it seems that the patient feels uncomfortable with the exam, take a moment to explore the reasons why. Discussing the exam in a-matter-of-fact way tends to lessen a patient's anxiety.
- As with all sensitive examinations, it is important to be mindful of the language used during the exam. While conducting the exam, tell the patient what you intend to do before actually performing the maneuver. In general, avoid words that can have intimate connotation, such as "feel", "touch", and "looks good", as well as words that are overly medical, such as "probe" and "palpate". Some useful neutral words include "examine", "check", "assess", "insert", and "appears healthy".
- Attempt to minimize exposure and expose only the area necessary to perform a thorough exam, then cover the patient as soon as the examination of that body part is completed. Avoid unnecessary physical contact, including inadvertent contact between your leg and the patient.
- If the patient is not already in a gown, ask them to change into one. Let the patient know you will leave the room while they change, and that you will knock prior to re-entry.
- Equipment
- Before beginning the exam, be sure everything needed is ready in advance. Prepare one pair of latex-free gloves, lubricant pre-expressed on a paper towel, a guaiac card and reagent (if checking for occult blood), a cotton swab (if doing a neurologic exam), and tissue paper to hand to the patient in order to clean up after the exam has ended.
- Physician Preparation
- Wash hands before beginning the exam.
- Before positioning or exposing the patient, put on your gloves and apply the lubricant to your dominant index finger. Apply a thin layer to the entire length and circumference of the finger. Applying too much leads to an unnecessary mess, while applying too little causes patient discomfort.
- It is helpful to engage in normal conversation with the patient while preparing, in order to minimize anxiety about the exam.
2. Performing the Exam
- Positioning the Patient
There are several acceptable ways to position a patient for the rectal exam:- In the first position, or Sims' position, have the patient lie down in the bed or on the exam table, and ask them to roll onto their left side with the left leg straight and the right leg flexed at the hip and knee. This is the preferred position for hospitalized patients and those unable to stand for the exam.
- In the second position, or modified lithotomy position, have the patient lie on their back with feet together and their hips and knees bent and abducted. This position may be useful in the hospitalized patient and may facilitate palpation of anterior structures, but limits inspection.
- In the third position, direct the patient to stand in front of the exam table with feet shoulder-width apart. Have the patient bend forward at the waist and support himself on his elbows and forearms. This is the preferred position in the office setting when the genitourinary (GU) exam will also be performed and for obese patients.
- Neurologic Assessment
- In the appropriate setting, it may be important to complete the neurological assessment with examination of perianal sensation, anal reflex, and sphincter tone. This is particularly important in patients for whom the diagnosis of cauda equina syndrome is being considered.
- Using a non-lubricated finger or cotton swab, gently touch the perianal region in a dermatomal pattern, and ask the patient to identify when you contact their skin.
- Test the anal reflex, an S2-S4 pathway, by using a non-lubricated finger to gently scratch the skin surrounding the anus, and observe for sphincter contraction.
- Assess the sphincter tone during the digital rectal exam (DRE).
- External Inspection and Palpation
- Carefully inspect the skin of the buttocks, sacrococcygeal, and perianal regions. To facilitate thorough inspection, either use the non-lubricated hand to separate the buttocks or ask the patient to reach back with the right hand and pull the right buttock forward.
- Carefully palpate any abnormal areas identified during perianal inspection.
- Digital Rectal Exam: Examination of Prostate and Rectum
- Inform the patient that, during the DRE, they may feel the urge to have a bowel movement. Reassure the patient that this is normal and an actual bowel movement will not occur.
- Ask the patient to bear or strain down, as if having a bowel movement.
- Quickly inspect the anus during the strain phase for prolapsing internal hemorrhoids or rectal tissue.
- Next, place the lubricated fingertip on the external anal sphincter, using gentle pressure, and pause.
- Once you feel the sphincter relax, fully insert the finger. If there is pain or the sphincter tightens, wait a moment and then continue once the sphincter has relaxed. Note sphincter tone during insertion. If there are concerns about sphincter tone, the clinical context calls for a complete neurologic assessment, ask the patient to squeeze down on your finger.
- Palpate the posterior surface of the prostate through the rectal wall, the apex of which is typically encountered 4-6 cm from the external anal sphincter. The prostate can be encountered by directing the finger anteriorly toward the umbilicus.
- Appreciate the median sulcus running between the lateral lobes of the prostate and follow it until the base of the prostate is felt. This may be beyond the length of the examiner's finger.
- Next, examine each lateral lobe of the prostate using abduction-adduction, flexion-extension, and supination-pronation movements of the finger. Use sufficient finger pressure to enhance detection of smaller lesions.
- Note relative symmetry of size, consistency, areas of nodularity, and tenderness. Use your fingertip to approximate the size of the prostate. Each fingertip-sized area is approximately 10-15 g.
- Next, with the finger fully inserted into the rectum, proceed to palpate the rectum.
- Begin by rotating the hand clockwise from six o'clock to one o'clock.
- Finally, rotate the hand counter-clockwise to twelve o'clock. In order to achieve this, the examiner must turn their body to the left, away from the patient. This is most easily done if the examiner is seated on a swivel chair or stool.
3. Completing the Exam
- After palpation of the rectum, withdraw your finger smoothly.
- Replace the gown to avoid exposing the patient for longer than necessary.
- Hand the patient tissue paper and invite him to clean himself.
- If a curtain is available, close it at this point to allow for privacy, otherwise turn your back to the patient until they are ready to continue.
- Inspect any stool that may be on your gloved hand for color, consistency, and blood. Use the guaiac card to test for occult blood, if indicated.
- Carefully dispose of the gloves and wash your hands.
- Once the patient is ready, review any normal and abnormal findings with him and discuss any next steps.
The male rectal exam remains an important part of the physical exam, particularly for patients with abdominal, genitourinary, or gastrointestinal concerns. Being a sensitive examination, it is extremely important that a physician knows how to conduct the steps in an appropriate manner, such that the patient's modesty is maintained without compromising the outcome of the exam.
Clinical indications for this exam include: lower urinary tract symptoms, urinary incontinence or retention, fecal incontinence or retention, back pain, anorectal symptoms, abdominal complaints, trauma patients, unexplained anemia, weight loss, or bone pain. This video will review the relevant anatomy of the male rectal area. And then it will provide the steps needed to conduct a comprehensive examination in a sensitive yet effective manner.
When performing the rectal exam, the examiner should conceptualize the relevant anatomy. The external anal sphincter is the most distal part of the anal canal. This canal is approximately three to four centimeters long and just beyond it lays the rectum, and anterior to the rectum is the prostate gland.
This gland is approximately 4 cm by 3.5 cm and 20-30 grams in a young man. Although its size normally increases with age. The posterior surface of the prostate, including its apex, base, median sulcus and lateral lobes, can be palpated through the rectal wall. The normal consistency of the prostate is similar to the thenar eminence when the hand is in a tight fist. The thumb knuckle is representative of what a hard nodule may feel like.
Now that we have reviewed the anatomy, let's discuss the essential steps of the examination. Inform the patient of the exam about to be performed and the reason for it. Recognize that some men may feel uncomfortable at the idea of having the exam performed. If it seems a patient feels uncomfortable with the exam, take a moment to explore the reasons why. Discussing the exam in a matter of fact way tends to lessen a patient's anxiety. As with all sensitive examinations, it is important to be mindful of the language used during the exam. While conducting the exam, tell the patient what you intend to do before actually performing the maneuver. In general, avoid words that can have intimate connotation, such as "feel", "touch", and "looks good", as well as words that are overly medical, such as "probe" and "palpate". Some useful neutral words include "examine", "check", "assess", "insert", and "appears healthy".
Before beginning the exam, be sure everything needed is ready in advance. Prepare one pair of latex-free gloves, lubricant pre-expressed on a paper towel, a cotton swab for neurologic examination, tissue paper for patient to clean self after the exam, and guaiac card and reagent-if testing for occult blood. Once the patient is comfortable, wash your hands and put on your latex-free gloves. Then, apply a thin layer of lubricant to your dominant index finger; be sure to apply enough lubricant to cover the entire length and circumference of the finger. Applying too much leads to an unnecessary mess, while applying too little causes patient discomfort.
Next, position the patient. There are three acceptable ways to position a patient for the rectal exam: the Sims' position, the modified lithotomy position and the standing position. For the Sim's position, have the individual lie down on the examination table. Then, instruct the patient to roll onto his left side with his left leg straight and right leg flexed at the hip and knee to 90°. Alternatively, both legs can be flexed at hips and knees to 90°. For modified lithotomy position, have the individual lie on his back with his feet together and hips and knees bent. For the third position, direct the patient to stand in front of the exam table with feet shoulder-width apart. Have the patient bend forward at the waist and support himself on his elbows and forearms. Throughout the procedure, expose only the area necessary to perform a thorough exam, and then cover the patient as soon as the examination of that body part is completed. Also, be careful to avoid unnecessary physical contact, including the inadvertent contact between your leg and the patient.
Begin by carefully inspecting the skin of the patient's buttocks, sacrococcygeal and perianal regions. Look for any ulcers, drainage, masses or nodules. You may use your hands to separate the buttocks, or you may ask the patient to reach back with his right hand and pull his right buttock forward. Be sure to carefully palpate any abnormal areas identified during your perianal inspection. In patients with neurologic symptoms or lower back pain, perform the neurological assessment of the perianal sensation. Using a cotton swab, gently touch the patient's perianal region in a dermatomal pattern. Ask the patient to notify you when you contact his skin.
Next, test the patient's anal reflex by using the cotton swab to gently scratch the skin surrounding the anus. Observe the sphincter for contraction. Following neurologic assessment, you should perform the digital rectal examination, which is mainly done to examine the prostate and the rectum. Inform the patient that he may feel the urge to have a bowel movement. And reassure that this is normal and an actual bowel movement will not occur.
First, ask your patient to bear or strain down, as if he was having a bowel movement. Next, with gentle pressure, place your lubricated fingertip on your patient's external anal sphincter, and pause. If the patient experiences pain or the sphincter tightens, then wait for a moment. Once you feel the sphincter relax, then fully insert your finger. Note the patient's sphincter tone during insertion. Ask the patient to squeeze down on your finger if the clinical context calls for a complete neurologic exam.
Next, palpate the posterior surface of the prostate through the patient's rectal wall. The prostate can be encountered by directing your finger anteriorly toward the umbilicus. Then locate the median sulcus, which runs between the lateral lobes of the prostate. Follow it until the base of the prostate is felt. This may be beyond the length of your finger. Examine each lateral lobe of the prostate using abduction, adduction, flexion, extension, supination and pronation movements of your finger. Use sufficient finger pressure to enhance detection of smaller lesions. Be sure to note the relative symmetry of size, consistency, areas of nodularity and tenderness. Use your fingertip to approximate the size of the prostate. Each fingertip-sized area is approximately 10-15 grams. Lastly, with your finger fully inserted, proceed to palpate the rectum. Begin by rotating your hand clockwise from six o'clock to one o'clock, and then back to the 6 o'clock position. Then, rotate your hand counter-clockwise to twelve o'clock by turning your body away from the patient.
Once complete, withdraw your finger smoothly and replace the gown to avoid exposing the patient for longer than necessary. Hand the patient tissue paper and invite him to clean himself. If a curtain is available, close it at this point to allow for privacy. Inspect any stool that may be on your gloved hand for color, consistency and blood. If necessary, use the guaiac card to test for occult blood. Then, carefully dispose of your gloves and wash your hands thoroughly. Once the patient is ready, review any normal and abnormal findings with him and discuss the subsequent steps to be taken, if necessary.
You have just watched a JoVE video documenting the male rectal examination. You should now understand the systematic sequence of steps every physician should follow in order to conduct an effective male rectal examination in a sensitive manner. As always, thanks for watching!
Subscription Required. Please recommend JoVE to your librarian.
Applications and Summary
The male rectal exam remains an important part of the physical exam, particularly for patients with abdominal, genitourinary, or gastrointestinal concerns. It is a sensitive procedure and requires careful attention to verbal and body language to ensure patient comfort. This video reviewed the indications and contraindications for the exam, relevant anatomy, as well the steps involved in performing the examination. Abnormalities that may be encountered at each step are found in Table 1. Physician comfort and technical proficiency with the rectal exam improves through practice, and the accuracy of the exam correlates with the experience of the examiner. As in other aspects of the physical exam, it is important to have a systematic method of examination. The method demonstrated in this video involves neurologic assessment, inspection and palpation of the perianal region, palpation of the prostate, palpation of the rectum, and finally, inspection of any stool on the gloved finger after the exam.

Table 1. Abnormalities detected during the male rectal exam. The table shows potential pathological findings that can be observed during rectal examination and their interpretations.
Limitations of the rectal exam are important to become familiar with. The rectum extends 12 to 15 cm beyond the anal canal, thus only the most distal portion can be palpated. Additionally, determining prostate size by DRE may be unreliable and thus should be considered an approximation. When compared with experienced urologists, students tend to palpate fewer areas of the prostate and use insufficient pressure, both of which limit detection of nodules. The examiner should always attempt to palpate the prostate from apex to base and both lateral lobes. However, with larger prostates, the examiner's finger may not be long enough to reach the base, limiting the evaluation. Finally, early malignancy is unlikely to be detected by DRE alone, thus screening for prostate cancer should be done with concomitant prostate specific antigen (PSA) testing in the appropriate patients.
Subscription Required. Please recommend JoVE to your librarian.