

ERRATUM NOTICE
Important: There has been an erratum issued for this article. Read more …
Summary
近年来,猪在研究中的使用有所增加。然而,猪的特点是气道解剖困难。通过演示如何进行内窥镜引导的气管插管,本协议旨在进一步提高实验动物的安全性,以避免动物痛苦和不必要的死亡。
Abstract
气管插管通常是猪模型中需要安全气道或高通气压的各种干预措施的转化研究的基本要求。气管插管是一项具有挑战性的技能,需要最少次数的成功气管插管才能在最佳条件下达到高成功率,这对于非麻醉学研究人员来说通常是无法实现的。由于猪气道解剖结构的特殊,通常可以假设气道困难。无法建立安全的气道可能导致实验动物受伤、不良事件或死亡。使用前瞻性、随机、对照评估方法,已经表明,光纤辅助气管插管需要更长的时间,但比传统插管具有更高的首过成功率,而不会引起临床相关的血氧饱和度下降。该模型为内镜引导的气管插管提供了一种标准化方案,提供了安全的气道,特别是对于在通过直接喉镜 进行 气管插管技术方面缺乏经验的研究人员。预计该程序将最大限度地减少动物痛苦和不必要的动物损失。
Introduction
气管插管通常是猪模型转化研究的基本要求,用于需要安全气道或高通气压(例如心肺复苏期间通气1或急性呼吸窘迫综合征2)或要求脑血流不会因声门上气道装置的内部压迫而受损的各种干预措施3,偶尔在猪4,5的预期困难气道背景下作为替代物传播。
虽然猪的肺生理学显示出与人类相似的特征6,但由于猪口腔解剖结构的特定差异,有时保护气道明显更困难7。猪的鼻子开口窄,舌头很大,喉部活动性极强,会厌相对较大,游离端延伸到软腭。在尾部,喉部与气管形成钝角。枸杞软骨大8.气道最窄的部分位于声门下9层,与儿童10的气道解剖结构相当。由于猪的喉部活动性很强,因此气管插管末端有可能穿过声带,但喉部只会在尾部移位几厘米,这可能会被误认为是正确的插管8,11。此外,在处理猪气道管理时,食管插管是一种常见风险12.
对实验或早期死亡率有相应负面影响的气管插管困难或不可能的发生率尚未系统记录,但已发表几份病例报告13,14。在人类中,有可能在意外困难的传统插管的情况下使用柔性插管内窥镜15。在采取这项措施之前,通常会进行各种假插管。这些反复插管尝试与人类的不良事件有关16,17,尤其是气道并发症18。这些事件在试验动物中是有害的,因为在最简单的情况下,它们代表了实验中的一个混杂变量;在最坏的情况下,它们可能导致不必要的动物损失。
本研究根据人类预期困难气道管理指南开发了一个模型15,19,20,21,22,23,24。以前,在人体研究中已经描述了用于学习光纤插管的类似技术25,26。本报告中提出的方案旨在提供一种标准化且易于适应的插管模型,该模型还允许非气道专家在猪中进行成功和安全的气管插管。
Subscription Required. Please recommend JoVE to your librarian.
Protocol
该协议中的实验得到了国家和机构动物护理委员会(Landesuntersuchungsamt Rheinland-Pfalz,科布伦茨,德国;批准号G20-1-135)的批准。实验是按照ARRIVE指南进行的。总体而言,本研究使用了10头平均体重为30公斤±2公斤,日龄为12-16周的麻醉公猪(Sus scrofa homea)。
1. 动物制备
- 为动物保持正常的环境,以尽量减少压力。在预定的实验前6小时停止进食以降低误吸风险,但允许获得水。
- 用针头(20 G)在臀肌或颈部联合注射咪达唑仑(0.5mg / kg)和氮哌隆(2-3mg / kg)(见 材料表)使猪镇静。让动物不受干扰,直到镇静开始(15-20分钟)。
注意:根据国家法规,镇静剂的管理可能会受到审查,并且可能需要也可能不需要训练有素的兽医的监督。在计划实验之前,请咨询地方当局。 - 将镇静动物从马厩运送到实验室。运输时间不得超过足够的镇静时间(此处为30-60分钟)。确保足够的保温性,使动物不会体温过低(即低于38°C),例如根据外部温度用毯子覆盖身体。
- 使用夹在耳朵或尾巴上的传感器(见 材料表),监测外周血氧饱和度(SpO2)。
- 在将外周静脉套管(22 G)插入耳静脉之前,用消毒剂(酒精)消毒皮肤。喷洒该区域,擦拭一次,然后再次喷洒,让消毒剂干燥。用创可贴固定耳套管(见材料表)。
2.麻醉和机械通气
- 通过静脉注射 4 μg/kg 芬太尼给予镇痛。通过静脉注射3mg / kg丙泊酚诱导麻醉(见 材料表)。
注意:由于推注,药物迅速涌入活动室,提供快速开始的深度麻醉。 - 将猪仰卧放在担架上,并用绷带固定。通过静脉注射0.5mg / kg阿曲库铵施用肌肉松弛剂(见 材料表)。
- 通过狗通气面罩(见材料表)或类似型号立即启动无创通气。为确保面罩紧密贴合,请将鱼际隆起和双手拇指放在面罩顶部,同时用其余手指进行下颌推力。
注意:通气参数:FiO 2(吸气氧分数)= 100%,吸气峰值压力= <20 cmH 2 0,呼吸频率=18-20次呼吸/分钟,PEEP(呼气末正压)= 5 cmH2 0。 - 通过连续输注0.1-0.2mg / kg / h芬太尼和8-12mg / kg / h丙泊酚来维持麻醉。开始连续注入 5 mL/kg/h 的平衡电解质溶液(参见 材料表)。不断保持足够的麻醉深度。
注意:这方面的替代参数是没有运动,插管后缺乏自己的呼吸努力,以及没有心率突然增加。如果可能,避免永久性肌肉松弛,以使运动反应成为麻醉深度不足的征兆。
3.气管插管
- 让助手站在头部的左侧。让助手的左手张开嘴,向外捏住舌头,然后用压缩来留下。让助手用右手食指向下按压右上唇,以提供更好的张嘴效果。
- 进行直接喉镜检查。为此,将喉镜(见 材料表)插入口腔右侧,并在将舌头向左推的同时向前推动。推进喉镜的尖端,直到它停留在声门瓣中。
注意:会厌通常粘附在软腭上,从而遮挡声门。 - 用管导丝(见 材料表)小心地将会厌推到一边,沿着软腭从右侧梨状凹槽向左侧轻轻舀取。
- 将喉镜的手柄传递给助手,将其固定在当前位置。
- 现在,使用柔性插管内窥镜,气管插管已经安装在上面,并连接到视频监视器。将内窥镜口服并推进到舌根,直到声门可见。
注意:为避免相机起雾,建议事先使用防雾剂(参见 材料表)。 - 将声带之间的内窥镜推进到气管中。通过目视识别软骨环和膜部来确认气管的解剖结构。推进内窥镜,直到它位于隆突上方。尽量不要用内窥镜的尖端触摸敏感的粘膜,以免肿胀和出血。
- 在保持内窥镜位置的同时,推进气管插管,直到它在相机图像中可见。
注意:如果气管插管无法通过声门平面推进,则有可能它已被卡在枸杞软骨上。在这种情况下,气管插管必须抽出 1 厘米并旋转 90°,然后再次轻轻推进。如有必要,可以重复此操作。类似口径的柔性插管内窥镜和气管插管可以将此问题发生的风险降至最低。如果尽管有这种操作仍无法推进气管插管,则声门下狭窄(猪喉最窄的部分)可能无法通过。在这种情况下,需要选择较小的气管插管尺寸。只要不存在解剖异常,内径为 6.5 cm 或 7.0 cm 的常规市售气管插管应该能够通过声门。气管插管尺寸要求因仔猪大小和品种而异。 - 取出柔性插管内窥镜,同时保持气管插管的位置。
- 使用 10 mL 注射器,用 10 mL 空气给袖带充气。使用气囊管理器控制气囊压力(目标值:30 cmH2O,参见 材料表)。
- 通过二氧化碳监测仪24定期和定期呼出二氧化碳和通过听诊15进行双面通气,确认气管插管的正确放置和充分通气。
- 将管子与呼吸机连接后开始机械通气(PEEP = 5 cmH 2 O,呼吸频率 = 可变以达到 <6 kPa 的潮气末 CO 2,通常为 30-50 min−1,FiO 2 = 0.4,I:E(吸气呼气比)= 1:2,潮气量 = 6-8 mL/kg)。
- 扩大监测(例如,建立动脉内血压测量,安装中心静脉或肺动脉导管27)或继续干预。
注意:根据进一步实验的问题,定义重要参数和干预选项的极限值,并在研究方案中相应地建立监测。
Subscription Required. Please recommend JoVE to your librarian.
Representative Results
在前瞻性、随机、对照研究环境中对10头公猪(12-16周龄,体重30公斤±3公斤)进行了气管插管。将猪随机分为两组:一组常规喉镜插管(CI组),另一组通过方案中描述的柔性插管内窥镜 辅助 插管(FIE组)。小组作业是通过拉密封的信封来完成的。研究者每天随机分配。
该研究由麻醉实习生进行,他们具有3年以上的麻醉经验,对人类气道管理有深刻的了解,并且在猪气管插管方面的经验少于7个月,麻醉护士协助插管并评估数据(n = 2,年龄:33岁±1年,人类气管插管经验: >1,000,人类清醒光纤插管:>100)。
FIE组按照上述方案进行了光纤辅助插管。CI组与FIE组的处理方式相同,直至协议的步骤3.2。之后,进行了以下更改。将喉镜插入声门瓣膜后,检查者用气管插管将会厌推到一边,气管插管中插入导丝,从右侧梨状肌凹槽沿软腭向左侧轻轻俯冲运动。之后,该气管插管在声带之间推进到气管中。导丝由助手抽出,用10mL注射器充气气管插管袖带,开始机械通气。
如果饱和度降至SpO2 93%以下或发生食管错位,则停止插管尝试,并进行面罩通气3分钟。在三次尝试失败后,从业者不得不改变程序。从喉镜检查开始计算每次试验的时间。
主要终点是第一次尝试插管的成功。次要终点是插管时间,测量为喉镜检查开始和呼吸机中检测到CO2 之间的时间,改变程序的需要以及使用声门开放百分比(POGO)量表评估气道。
使用市售软件进行统计分析(见 材料表)。使用柯尔莫哥罗夫-斯米尔诺夫检验28检查正态分布。如果确定正态分布,则使用独立样本29 的 t 检验或非参数版本的曼-惠特尼 U 检验30 分析组差异。数据以平均值(±标准差)表示。使用斯皮尔曼相关系数31 检查序数尺度数据的相关性。假设显著性水平为 p < 0.05。所有测试都是出于探索性意图进行的;因此,p 值是描述性的。尽管如此,p < 0.05被接受为统计显著性的指标。
FIE组在第一次尝试时表现出比CI组更高的成功率趋势(100%对60%);总体而言,FIE组需要的插管尝试较少(1.0 ± 0 vs 1.4 ± 0.548, p = 0.310)(图1)。在任何情况下,饱和度都不会降至93%以下,因此无需更改程序。需要第二次尝试插管,因为声门下狭窄的通过不可能顺利(n = 1)和食管错位(n = 1)。
总体而言,FIE组成功的插管尝试时间明显长于CI组(71.2 s ± 18.336 s vs. 36.8 s ± 18.472 s,p = 0.018)。一般来说,声门很容易可视化,具有良好的可见性(POGO:77%±27.1%),没有组别差异(FIE 86% ± 26.077% vs. CI 68% ± 27.749%,p = 0.513)。在常规插管组(CI)中,需要更多的气管插管尝试,但这无统计学意义(1.0 ± 0 vs. 1.4 ± 0.548,p = 0.310)。在内窥镜引导的插管组(FIE)中,呼吸机中检测到CO 2需要更长的时间(71.2 s ± 18.336 s vs. 36.8 s ± 18.472 s,p = 0.018)(图2)。

图 1:组比较中的插管尝试次数。 对于使用柔性插管内窥镜插管的组,每次插管尝试都成功;在常规插管组中,平均需要1.4次尝试才能正确放置气管插管。误差线显示标准偏差。n = 5(每组)。请点击此处查看此图的大图。

图 2:组比较中检测到 CO2 的时间。 对于使用柔性插管内窥镜插管的组,在检测到潮气末CO2之前需要更长的时间,描述为平均值和标准偏差。n = 5(每组)。请点击此处查看此图的大图。
Subscription Required. Please recommend JoVE to your librarian.
Discussion
在之前的研究中,我们的研究小组已经描述了有关猪模型2,27,32,33的转化益处的具体细节。一般来说,降低动物的压力水平和不必要的疼痛应该是任何研究方案的一个组成部分,对于产生可靠的可重复数据至关重要。因此,对预期气道困难的猪进行清醒内镜引导的插管不是一种选择。
必须指出的是,大型动物模型中的诱导和维持麻醉只能由经过专门培训的人员或在其直接监督下进行。在计划和进行此类实验时不遵守此规则可能会导致动物的相关伤害、疼痛、压力、焦虑或死亡。需要正确定位猪,以确保充分通气、充分喉镜检查和成功插管。仰卧位便于轻松访问所呈现的气道管理方案,并在必要时允许后续仪器,而无需重新定位动物8。
尽管需要避免多次插管尝试,但在插管尝试失败的情况下恢复面罩通气至关重要。当血氧饱和度降至 93% 以下时,建议停止插管尝试。必须如上所述通过面罩通气 进行 预氧合,以提供足够的氧气储备。
为了使气管插管尽可能轻柔地通过声门开口,必须避免内窥镜和插管之间的口径跳跃过大。否则,被大软骨卡住的风险更高8。软式插管内镜辅助气管插管需要更长的时间,但首次尝试成功率更高。作者将首次插管尝试成功率缺乏统计学意义归因于病例数量少。根据作者的经验,假插管是一种常见的风险,特别是如果非麻醉师在培训中(例如博士生)进行插管。食管插管在这里介绍的研究集体中发生过一次,这是可能的,因为气管插管在直接喉镜检查下完全覆盖了声门视图,因为插入视野后气道相对狭窄。在最初的两次不成功的尝试中,插管器能够通过重新定位喉镜来创造更好的插管条件。
增加的持续时间在该队列中没有临床意义。在任何时候都没有达到终止标准 - 饱和度低于93%。这显示在结果中,因为任何时候都不需要更改过程。事先进行充分的面罩通气是留出足够时间放置光纤气管插管以避免快速去饱和的关键步骤34。这些结果与先前比较传统插管和内镜辅助插管与缺乏经验的提供者的研究一致35。我们将光纤插管持续时间延长归因于这样一个事实,即插入后必须首先重新定向,而对于常规插管,人们保留了声门的视野。在推进过程中,避免使用柔性插管内窥镜与粘膜接触也很重要。这需要偶尔的纠正操作。最后但并非最不重要的一点是,成功放置后,需要缩回相对较长的内窥镜,这略微增加了CO2 检测的时间。
所呈现结果的局限性在于,进行研究的参与者是具有高水平气道专业知识的麻醉师。对于具有代表性的结果,我们选择该研究集体作为研究者,以防止通过学习效应36混淆变量。人类需要成功插管50多次才能达到90%以上的成功率37。对于非麻醉师来说,这些数字通常是不可能的。
与人类相比,猪的气道可能很困难7,8,9。对于非麻醉师来说,预计失败率甚至高于这些结果。与人类气管插管的学习曲线相比,猪柔性内镜插管的可学习性似乎更容易获得35。与传统喉镜检查相比,它还具有优势,只要使用视频监视器,主管就可以立即识别插管失败。因此,建议使用连接到柔性插管内窥镜的高分辨率监视器,尤其是在首次使用该技术时。这使得监督变得更加容易,并增加了执行它的人的学习效果,因为主管可以在不自己接管任务的情况下调节技术。在食管插管(最常见的并发症12)的情况下,由于听诊可能呈假阳性,因此问题通常只有在通过缺失的二氧化碳图曲线进行胃通气后才会变得明显38。反过来,臃肿的胃在人类中具有缺点,即功能残余能力因此而降低,随后的插管尝试可能导致饱和度更快地下降39。
根据作者的经验,猪的面罩通风很容易实现。然而,在多次尝试失败后,不良事件的发生率显着增加16,并且在多次尝试后气管插管本身也变得越来越困难40。与人类不同,根据研究设计,使用声门外气道装置或恢复自主呼吸15 的替代气道管理是不合理的。因此,应始终以气管插管尝试次数最少为目标,以确保气道安全。
与考虑传统气管插管相当困难的学习性相反,使用柔性插管内窥镜的气管插管被错误地认为难以学习41。据作者所知,在喉镜的帮助下使用柔性插管内窥镜在麻醉患者中进行气管插管的学习曲线从未得到系统研究。Johnson等人42 在系统研究中表明,10次清醒内镜引导的气管插管足以对人体进行安全,令人满意的插管内窥镜检查。然而,这适用于自主呼吸的清醒患者,他们带来了自己的困难程度(足够的镇静,明显的咳嗽冲动,上呼吸道的肿瘤变化等)。库克等人36 也得出了类似的结论。在没有这些加重情况的情况下,预计没有其他相关气道病变的麻醉猪的学习曲线会更陡峭。人类的学习曲线从第五次插管开始明显变平(Cook et al.36, Johnson et al.42)。与传统插管相比,这是一个更陡峭的学习曲线。
Ruemmler等人35 能够证明,内窥镜辅助气管插管是一种在简短介绍后相对容易为有指导的初学者执行的程序。新手在内窥镜引导的气管插管方面甚至比这里介绍的研究中的麻醉师更快。新手在所有病例中都设法独立保护气道,而在传统气管插管的病例中,他们有13%需要帮助。因此,柔性内窥镜辅助气管插管是传统气管插管的安全替代方案,其侵入性明显小于例如经皮气管切开术和自主呼吸,后者在以前的研究中提出43。由于猪的依从性有限,自主呼吸下充分吸氧的可能性很低,本报告的作者认为,如果需要气管插管,内镜辅助气管插管是猪替代气道管理最安全的变体。虽然并非每个研究小组都可以使用柔性插管内窥镜或使用它们,但那些这样做的研究小组可以提供更多的动物安全性。例如,在正在进行的试验中防止动物损失以及在多次试验中重复使用它们的潜力,通常比购买一次性柔性插管内窥镜的经济挑战所抵消。
该实验方案为猪内镜辅助气管插管提供了标准化程序。此设置可为需要气管插管的各种实验提供安全的气道管理。这有助于减少动物的痛苦和不必要的损失的可能性。
Subscription Required. Please recommend JoVE to your librarian.
Disclosures
柔性插管内窥镜及其配件由制造商无条件提供,仅用于研究目的。提交人声明没有进一步的财务或其他利益冲突。
Acknowledgments
作者要感谢Dagmar Dirvonskis的出色技术支持。
Materials
| Name | Company | Catalog Number | Comments |
| Ambu aScope Regular | Ambu GmbH, Medizinprodukte, Bad Nauheim, Germany | Disposable fiber optic outer diameter 5 mm | |
| Ambu aView Monitor | Ambu GmbH, Medizinprodukte, Bad Nauheim, Germany | monitor | |
| Atracurium Hikma 50 mg/5mL | Hikma Pharma GmbH, Martinsried | atracurium | |
| Azaperone (Stresnil) 40mg/mL | Lilly Deutschland GmbH, Bad Homburg, Germany | azaperone | |
| BD Discardit II Spritze 2, 5, 10, 20 mL | Becton Dickinson S.A. Carretera, Mequinenza Fraga, Spain | syringe | |
| BD Luer Connecta | Becton Dickinson Infusion Therapy, AB Helsingborg, Schweden | 3-way-stopcock | |
| BD Microlance 3 20 G | Becton Dickinson S.A. Carretera, Mequinenza Fraga, Spain | cannula | |
| Curafix i.v. classics | Lohmann & Rauscher International GmbH & Co. KG, Rengsdorf, Germany | Cannula retention dressing | |
| Engström Carestation | GE Heathcare, Madison USA | ventilator | |
| Fentanyl-Janssen 0.05 mg/mL | Janssen-Cilag GmbH, Neuss | fentanyl | |
| Führungsstab, Durchmesser 4.3 | Rüsch | endotracheal tube introducer | |
| IBM SPSS Statistics for Windows, Version 20 | IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.) | Statistical software | |
| Incetomat-line 150 cm | Fresenius, Kabi Deutschland, GmbH | perfusor line | |
| Intrafix Primeline | B. Braun Melsungen AG, Melsungen, Germany | Infusion line | |
| JOZA Einmal Nitril Untersuchungshandschuhe | JOZA, München, Germany | disposable gloves | |
| Laryngoscope, 45.48.50, KL 2000 | Medicon | Laryngoscope handle | |
| Littmann Classic III Stethoscope | 3M Deutschland GmbH, Neuss, Germany | stethoscope | |
| Luer Lock | B.Braun Melsungen AG, Germany | ||
| Maimed Vlieskompresse | Maimed GmbH, Neuenkirchen, Germany | Fleece compress to fix the tongue | |
| Masimo LNCS Adtx SpO2 sensor | Masimo Corporation Irvine, Ca 92618 USA | saturation clip for the tail | |
| Masimo LNCS TC-I SpO2 ear clip sensor | Masimo Corporation Irvine, Ca 92618 USA | Saturation clip for the ear | |
| Masimo Radical 7 | Masimo Corporation Irvine, Ca 92618 USA | periphereal oxygen saturation | |
| Midazolam 15 mg/3 mL | Hameln Pharma GmbH, Hameln, Germany | midazolam | |
| Midmark Canine Mask Small Plastic with Diaphragm FRSCM-0005 | Midmark Corp., Dayton, Ohio, USA | dog ventilation mask | |
| Octeniderm farblos | Schülke & Mayr GmbH, Nordenstedt, Germany | Alcoholic disinfectant | |
| Original Perfusor syringe 50 mL | B.Braun Melsungen AG, Germany | perfusor syringe | |
| Perfusor FM Braun | B.Braun Melsungen AG, Germany | syringe pump | |
| Propofol 2% 20 mg/mL (50 mL flasks) | Fresenius, Kabi Deutschland, GmbH | propofol | |
| RÜSCH Führungsstab für Endotrachealtubus (ID 5.6 mm) | Teleflex Medical Sdn. Bhd, Malaysia | PVC coated tube guiding wire | |
| Rüschelit Super Safety Clear >ID 6/6.5 /7.0 mm | Teleflex Medical Sdn. Bhd, Malaysia | endotracheal tube | |
| Stainless Macintosh Größe 4 | Welch Allyn69604 | blade for laryngoscope | |
| Sterofundin | B.Braun Melsungen AG, Melsungen, Germany | Balanced electrolyte solution | |
| Ultrastop Antibeschlagmittel bottle with dropper 25 mL | Sigmapharm Arzneimittel GmbH, Wien, Austria | Antifog agent | |
| Vasofix Safety 22 G-16 G | B.Braun Melsungen AG, Germany | venous catheter | |
| VBM Cuff Manometer | VBM Medizintechnik GmbH, Sulz a.N., Germany | cuff pressure gauge | |
| Zelette | Lohmann & Rauscher International GmbH & Co. KG, Rengsdorf, Germany | Tissue swab |
References
- Kleinman, M. E., Oh, W., Stonestreet, B. S. Comparison of intravenous and endotracheal epinephrine during cardiopulmonary resuscitation in newborn piglets. Critical Care Medicine. 27 (12), 2748-2754 (1999).
- Rissel, R., et al. Bronchoalveolar lavage and oleic acid-injection in pigs as a double-hit model for acute respiratory distress syndrome (ARDS). Journal of Visualized Experiments. (159), e61358 (2020).
- Segal, N., et al. Impairment of carotid artery blood flow by supraglottic airway use in a swine model of cardiac arrest. Resuscitation. 83 (8), 1025-1030 (2012).
- Goldmann, K., Kalinowski, M., Kraft, S. Airway management under general anaesthesia in pigs using the LMA-ProSeal: A pilot study. Veterinary Anaesthesia and Analgesia. 32 (5), 308-313 (2005).
- Wemyss-Holden, S. A., Porter, K. J., Baxter, P., Rudkin, G. E., Maddern, G. J. The laryngeal mask airway in experimental pig anaesthesia. Lab Animal. 33 (1), 30-34 (1999).
- Kobayashi, E., Hishikawa, S., Teratani, T., Lefor, A. T. The pig as a model for translational research: overview of porcine animal models at Jichi Medical University. Transplantation Research. 1 (1), 8 (2012).
- Judge, E. P., et al. Anatomy and bronchoscopy of the porcine lung. A model for translational respiratory medicine. American Journal of Respiratory Cell and Molecular Biology. 51 (3), 334-343 (2014).
- Dondelinger, R. F., et al. Relevant radiological anatomy of the pig as a training model in interventional radiology. European Radiology. 8 (7), 1254-1273 (1998).
- Nickel, R., Schummer, A., Seiferle, E. Lehrbuch der Anatomie der Haustiere, Band I: Bewegungsapparat. , Parey. Singhofen, Germany. (2003).
- Wani, T. M., Rafiq, M., Akhter, N., AlGhamdi, F. S., Tobias, J. D. Upper airway in infants-A computed tomography-based analysis. Paediatric Anaesthesia. 27 (5), 501-505 (2017).
- Chum, H., Pacharinsak, C.
- Ettrup, K. S., et al. Basic surgical techniques in the Göttingen minipig: Intubation, bladder catheterization, femoral vessel catheterization, and transcardial perfusion. Journal of Visualized Experiments. (52), e2652 (2011).
- Steinbacher, R., von Ritgen, S., Moens, Y. P. S. Laryngeal perforation during a standard intubation procedure in a pig. Laboratory Animals. 46 (3), 261-263 (2012).
- Iliff-Sizemore, S. A., Chrisp, C. E., Rush, H. G. Peritracheolaryngeal abscess: An iatrogenic complication of endotracheal intubation in swine. Laboratory Animal Science. 39 (5), 455-458 (1989).
- Piepho, T., et al. S1 guidelines on airway management. Der Anaesthesist. 64 (11), 859-873 (2015).
- Mort, T. C. Emergency tracheal intubation: Complications associated with repeated laryngoscopic attempts. Anesthesia & Analgesia. 99 (2), 607-613 (2004).
- Hasegawa, K., et al. Association between repeated intubation attempts and adverse events in emergency departments: An analysis of a multicenter prospective observational study. Annals of Emergency Medicine. 60 (6), 749-754 (2012).
- Martin, L. D., Mhyre, J. M., Shanks, A. M., Tremper, K. K., Kheterpal, S. 3,423 emergency tracheal intubations at a university hospital: airway outcomes and complications. Anesthesiology. 114 (1), 42-48 (2011).
- Ahmad, I., et al. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia. 75 (4), 509-528 (2020).
- Frerk, C., et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British Journal of Anaesthesia. 115 (6), 827-848 (2015).
- Cook, T. M., et al. Consensus guidelines for managing the airway in patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia. 75 (6), 785-799 (2020).
- Kornas, R. L., Owyang, C. G., Sakles, J. C., Foley, L. J., Mosier, J. M. Evaluation and management of the physiologically difficult airway: Consensus recommendations from Society for Airway Management. Anesthesia & Analgesia. 132 (2), 395-405 (2021).
- Higgs, A., et al. Guidelines for the management of tracheal intubation in critically ill adults. British Journal of Anaesthesia. 120 (2), 323-352 (2018).
- Apfelbaum, J. L., et al. American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 136 (1), 31-81 (2022).
- Doyle, D. J. GlideScope-assisted fiberoptic intubation: A new airway teaching method. Anesthesiology. 101 (5), 1252 (2004).
- Lenhardt, R., et al. Is video laryngoscope-assisted flexible tracheoscope intubation feasible for patients with predicted difficult airway? A prospective, randomized clinical trial. Anesthesia & Analgesia. 118 (6), 1259-1265 (2014).
- Ruemmler, R., Ziebart, A., Garcia-Bardon, A., Kamuf, J., Hartmann, E. K. Standardized model of ventricular fibrillation and advanced cardiac life support in swine. Journal of Visualized Experiments. (155), e60707 (2020).
- Dodge, Y. Kolmogorov-Smirnov Test. The Concise Encyclopedia of Statistics. , Springer. New York, NY. 283-287 (2008).
- Ross, A., Willson, V. L. Independent Samples T-test. Basic and Advanced Statistical Tests: Writing Results Sections and Creating Tables and Figures. , SensePublishers. Rotterdam, The Netherlands. 13-16 (2017).
- Mann, H. B., Whitney, D. R. On a test of whether one of two random variables is stochastically larger than the other. The Annals of Mathematical Statistics. 18 (1), 50-60 (1947).
- Spearman, C. The proof and measurement of association between two things. American Journal of Psychology. 100 (3-4), 441-471 (1987).
- Ziebart, A., et al. Standardized hemorrhagic shock induction guided by cerebral oximetry and extended hemodynamic monitoring in pigs. Journal of Visualized Experiments. (147), e59332 (2019).
- Kamuf, J., et al. Oleic acid-injection in pigs as a model for acute respiratory distress syndrome. Journal of Visualized Experiments. (140), e57783 (2018).
- Kurita, T., Kawashima, S., Morita, K., Nakajima, Y. Assessment of the benefits of head-up preoxygenation using near-infrared spectroscopy with pulse oximetry in a swine model. Journal of Clinical Monitoring and Computing. 35 (1), 155-163 (2021).
- Ruemmler, R., Ziebart, A., Ott, T., Dirvonskis, D., Hartmann, E. K. Flexible fibreoptic intubation in swine - Improvement for resident training and animal safety alike. BMC Anesthesiology. 20 (1), 206 (2020).
- Cook, J. A., Ramsay, C. R., Fayers, P. Using the literature to quantify the learning curve: A case study. International Journal of Technology Assessment in Health Care. 23 (2), 255-260 (2007).
- Buis, M. L., Maissan, I. M., Hoeks, S. E., Klimek, M., Stolker, R. J. Defining the learning curve for endotracheal intubation using direct laryngoscopy: A systematic review. Resuscitation. 99, 63-71 (2016).
- Knapp, S., et al. The assessment of four different methods to verify tracheal tube placement in the critical care setting. Anesthesia & Analgesia. 88 (4), 766-770 (1999).
- Schmidt, R. F. Physiologie des Menschen. 31, Springer. New York, NY. (2010).
- Eberlein, C. M., Luther, I. S., Carpenter, T. A., Ramirez, L. D. First-pass success intubations using video laryngoscopy versus direct laryngoscopy: A retrospective prehospital ambulance service study. Air Medical Journal. 38 (5), 356-358 (2019).
- Lohse, J., Noppens, R. Awake video laryngoscopy - An alternative to awake fiberoptic intubation. Anasthesiologie, Intensivmedizin, Notfallmedizin, Schmerztherapie. 51 (11-12), 656-663 (2016).
- Johnson, C., Roberts, J. T. Clinical competence in the performance of fiberoptic laryngoscopy and endotracheal intubation: A study of resident instruction. Journal of Clinical Anesthesia. 1 (5), 344-349 (1989).
- Geovanini, G. R., Pinna, F. R., Prado, F. A., Tamaki, W. T., Marques, E. Standardization of anesthesia in swine for experimental cardiovascular surgeries. Revista Brasileira de Anestesiologia. 58 (4), 363-370 (2008).
Tags
医学,第 186 期,气道管理,猪,动物模型,气管插管,光纤Erratum
Formal Correction: Erratum: Endotracheal Intubation Using a Flexible Intubation Endoscope As a Standardized Model for Safe Airway Management in Swine
Posted by JoVE Editors on 04/03/2023.
Citeable Link.
An erratum was issued for: Endotracheal Intubation Using a Flexible Intubation Endoscope As a Standardized Model for Safe Airway Management in Swine. The Protocol, Representative Results, and Discussion sections were updated.
In the Protocol, step 1.5 was updated from:
Disinfect the skin with a disinfectant (alcoholic) before inserting a peripheral vein cannula (22 G) into an ear vein. Spray the area, wipe once, then spray again, and allow the disinfectant to dry.
to:
Disinfect the skin with a disinfectant (alcoholic) before inserting a peripheral vein cannula (22 G) into an ear vein. Spray the area, wipe once, then spray again, and allow the disinfectant to dry. Secure the ear cannula with a band-aid (See Table of Materials).
In the Protocol, step 3.7 was updated from:
While maintaining the position of the endoscope, advance the endotracheal tube until it becomes visible in the camera image.
NOTE: If the endotracheal tube cannot be advanced through the glottic plane, there is a possibility that it has become caught on the arytenoid cartilage. In this case, the endotracheal tube must be withdrawn 1 cm and rotated by 90° before gently advancing again. If necessary, this maneuver can be repeated. Similar calibers of flexible intubation endoscope and endotracheal tube can minimize the risk of this issue occurring. If the endotracheal tube cannot be advanced despite this maneuver, it is likely that the subglottic narrowness-the narrowest part of the porcine larynx-cannot be passed. In this case, a smaller endotracheal tube size needs to be selected. Regular commercially available endotracheal tubes in sizes 6.5 cm or 7.0 cm ID should be able to pass the glottis as long as no anatomic abnormalities are present.
to:
While maintaining the position of the endoscope, advance the endotracheal tube until it becomes visible in the camera image.
NOTE: If the endotracheal tube cannot be advanced through the glottic plane, there is a possibility that it has become caught on the arytenoid cartilage. In this case, the endotracheal tube must be withdrawn 1 cm and rotated by 90° before gently advancing again. If necessary, this maneuver can be repeated. Similar calibers of flexible intubation endoscope and endotracheal tube can minimize the risk of this issue occurring. If the endotracheal tube cannot be advanced despite this maneuver, it is likely that the subglottic narrowness-the narrowest part of the porcine larynx-cannot be passed. In this case, a smaller endotracheal tube size needs to be selected. Regular commercially available endotracheal tubes in sizes 6.5 cm or 7.0 cm ID should be able to pass the glottis as long as no anatomic abnormalities are present. Endotracheal tube size requirements vary depending on the piglet size and breed.
In the Representative Results, the sixth paragraph was updated from:
Statistical analyses were performed using commercially available software (see Table of Materials). Normal distribution was examined using the Kolmogorov-Smirnoff test28. If a normal distribution was determined, group differences were analyzed using t-tests of independent samples29 or the Mann-Whitney U test30 for the non-parametric version. Data are presented as mean (± standard deviation). Correlations of ordinal-scale data were examined using Spearman's correlation coefficient31. A significance level of p < 0.05 was assumed.
to:
Statistical analyses were performed using commercially available software (see Table of Materials). Normal distribution was examined using the Kolmogorov-Smirnoff test28. If a normal distribution was determined, group differences were analyzed using t-tests of independent samples29 or the Mann-Whitney U test30 for the non-parametric version. Data are presented as mean (± standard deviation). Correlations of ordinal-scale data were examined using Spearman's correlation coefficient31. A significance level of p < 0.05 was assumed. All tests were performed with exploratory intention; therefore p-values are descriptive. Nevertheless, p < 0.05 was accepted as indicative of statistical significance.
In the Representative Results, the legend for figure 1 was updated from:
Figure 1: Number of intubation attempts in group comparison. For the group that was intubated using a flexible intubation endoscope, every intubation attempt was successful; in the group that was conventionally intubated, it took an average of 1.4 attempts before the endotracheal tube could be placed correctly. Error bars show the standard deviation. Please click here to view a larger version of this figure.
to:
Figure 1: Number of intubation attempts in group comparison. For the group that was intubated using a flexible intubation endoscope, every intubation attempt was successful; in the group that was conventionally intubated, it took an average of 1.4 attempts before the endotracheal tube could be placed correctly. Error bars show the standard deviation. n = 5 (for each group). Please click here to view a larger version of this figure.
In the Representative Results, figure 2 was updated from:
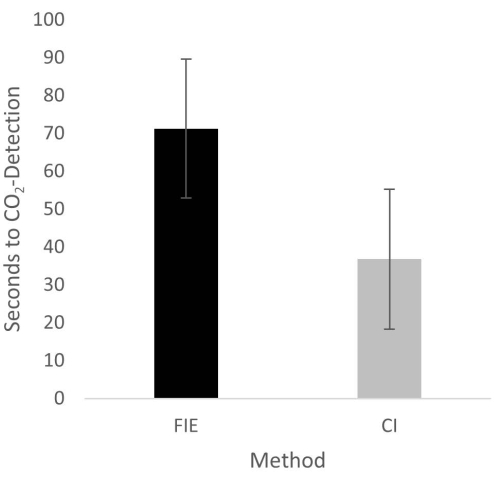
Figure 2: Time until CO2 detection in group comparison. For the group that was intubated using a flexible intubation endoscope, it took significantly longer until end-tidal CO2 could be detected, depicted as mean and standard deviation. Please click here to view a larger version of this figure.
to:
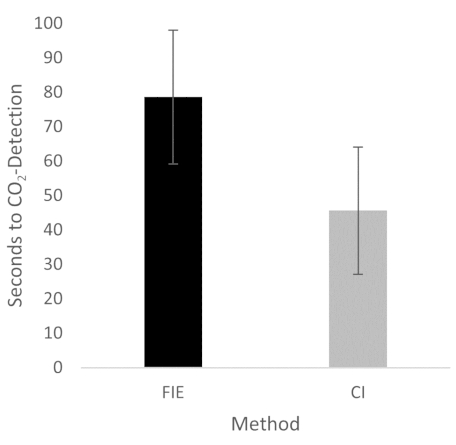
Figure 2: Time until CO2 detection in group comparison. For the group that was intubated using a flexible intubation endoscope, it took significantly longer until end-tidal CO2 could be detected, depicted as mean and standard deviation. n = 5 (for each group). Please click here to view a larger version of this figure.
In the Discussion, the fifth paragraph was updated from:
The increased duration had no clinical significance in this cohort. At no time was the termination criterion-a saturation of less than 93%-reached. This is shown in the results because a procedure change was unnecessary at any time. Prior adequate mask ventilation is a critical step to allow sufficient time for fiberoptic endotracheal tube placement to avoid rapid desaturation34. These results are consistent with previous studies comparing conventional intubation and endoscopically assisted intubations with inexperienced providers35.
to:
The increased duration had no clinical significance in this cohort. At no time was the termination criterion-a saturation of less than 93%-reached. This is shown in the results because a procedure change was unnecessary at any time. Prior adequate mask ventilation is a critical step to allow sufficient time for fiberoptic endotracheal tube placement to avoid rapid desaturation34. These results are consistent with previous studies comparing conventional intubation and endoscopically assisted intubations with inexperienced providers35. We attribute the prolonged duration of fiberoptic intubation to the fact that one must first reorient again after insertion, whereas with conventional intubation, one retains a view of the glottis. It is also important to avoid contact with the mucosa with the flexible intubation endoscope during advancement. This requires occasional corrective maneuvers. Last but not least, after successful placement, retraction of the relatively long endoscope is required, which increases the time to CO2 detection slightly.
