

Summary
This manuscript describes a method for continuous video EEG recordings using multiple depth electrodes in neonatal mice undergoing hypoxia-ischemia.
Abstract
Hypoxia ischemia is the most common cause of neonatal seizures. Animal models are crucial for understanding the mechanisms and physiology underlying neonatal seizures and hypoxia ischemia. This manuscript describes a method for continuous video electroencephalogram (EEG) monitoring in neonatal mice to detect seizures and analyze EEG background during hypoxia ischemia. Use of video and EEG in conjunction allows description of seizure semiology and confirmation of seizures. This method also allows analysis of power spectrograms and EEG background pattern trends over the experimental time period. In this hypoxia ischemia model, the method allows EEG recording prior to injury to obtain a normative baseline and during injury and recovery. Total monitoring time is limited by the inability to separate pups from the mother for longer than four hours. Although, we have used a model of hypoxic-ischemic seizures in this manuscript, this method for neonatal video EEG monitoring could be applied to diverse disease and seizure models in rodents.
Introduction
Hypoxic ischemic encephalopathy (HIE) is a condition that affects 1.5 in 1000 newborns annually and is the most common cause of neonatal seizures1,2. Infants who survive are at risk for various neurological disabilities such as cerebral palsy, intellectual disability, and epilepsy3,4,5.
Animal models play a critical role in understanding and investigating the pathophysiology of hypoxia ischemia and neonatal seizures6,7. A modified Vannucci model is used to induce hypoxia ischemia (HI) on postnatal day 10 (p10)7,8. Mouse pups of this age translate neurologically roughly to the full term human neonate9.
Continuous video electroencephalography (EEG) monitoring used in conjunction with this injury model allows for further understanding and characterization of neonatal hypoxic ischemic seizures. Previous studies have used various methods for analyzing neonatal seizures in rodents, including video recordings, limited EEG recordings and telemetry EEG recordings10,11,12,13,14,15,16. In the following manuscript, we discuss in depth the process of recording continuous video EEG in mouse pups during hypoxia-ischemia. This technique for continuous video EEG monitoring in neonatal mouse pups could be applied to a variety of disease and seizure models.
Subscription Required. Please recommend JoVE to your librarian.
Protocol
All animal studies were approved by the Institutional Animal Care and Use Committee (IACUC) of the University of Virginia.
1. Electrode building/cable building
- Use a unipolar insulated stainless-steel wire (0.005” bare diameter, 0.008” coated) to make an electrode that is connected with a female socket connector (female receptacle connector 0.079).
- Use a special custom-made cable to connect animals to the amplifier.
- Attach a male 4-pin connector (Male connector 0.079”) to 4 channel unity gain impedance matching operational amplifier (op-amp). Attach a 10K resistor to the wires that connect to the 9 V battery. A ground wire not connected to the op-amp acts as the midpoint of the battery.
- Connect one end of the cable (AWG, 0.012” OD) to the op-amp and connect the other end of the cable to the amplifier.
2. Electrode implantation surgery
- Anesthetize the pup (postnatal day 9) with 4-5% isoflurane in a downward flow hood. Prior to the start of the procedure, inject the pups with bupivacaine (0.02-0.05 mL, 0.25% subcutaneous local infiltration).
- Once the animal is immobile, transfer to a stereotactic stage with a nose cone. Use the reverse side of the ear bar as it is soft to hold the head steady. At this age, pups do not have a fully developed ear to use the pointed end of the ear bar.
- Turn down the flow of isoflurane and maintain it at 2.5-3%. Keep an eye on steady breathing of the pup throughout the surgery procedure. Pinch the tail to check pain response and then proceed to incision.
- Sterilize the incision area on the skull with betadine and alcohol (3 cycles of alternating iodine and 70% ethanol). Drape the surrounding body part such that the incision region is visible.
- Open the scalp anterior-posterior from slightly above the eyes and retract approximately 0.5 cm of skin. Reposition the mouse head on the stereotaxic stage so that the skin pulls outward exposing skull.
- Apply hydrogen peroxide on the skull using a cotton swab and scrape the skull clean using a scalpel blade. The skull is very soft; exercise caution while scraping.
- Apply one drop (approximately 50 µL) of adhesive and spread it around the exposed skull area using its applicator. Expose to UV light for 40 s to set the adhesive.
- Measure the coordinates using the exposed bregma as the reference. Implant electrodes bilaterally in the CA1 region of hippocampus [-3.5 mm Dorsal-Ventral (DV), ±2 mm Medial-Lateral (ML), -1.75 mm Deep (D)] and bilaterally in the parietal cortex [-1.22 mm DV, ±0.5 mm ML, -1 mm D] and a reference electrode in the cerebellum17. Use a 32 G needle to create a hole at the marked region.
- Clean the blood from the surface of the skull. Lower electrodes attached to the female socket connector into the brain with the help of the stereotaxic arm and fix in place with dental acrylic. Implant the electrode in the brain. The socket connector headset sits on top of the skull glued together by dental acrylic.
- Inject ketoprofen (5 mg/kg) subcutaneously in the interscapular region once the electrode is fixed. Place the pups back with the mother.
NOTE: Introduce half of the litter with the headset at once to the mother rather than introducing them one at a time. This will prevent from mother damaging the pup’s headset.
3. EEG setup and recording (baseline/pre-injury)
- After 24 h of recovery after electrode implantation, place each animal in a heated (37 °C) custom-made Plexiglas chamber for EEG recording. This chamber will also serve as a hypoxia chamber.
- Connect pups in the chamber to a video-EEG monitoring system via a flexible cable (custom made op-amp cable).
NOTE: With the headset in place, the mice are freely mobile and do not exhibit any differences in behavior. Once attached to the electrode wires, the wires must be adjusted within the chamber tether in order to provide the right amount of slack so that the pup can freely move throughout the chamber. - Digitize the EEG data at 1000 Hz with 1K gain using a grass amplifier. Review the EEG signal (band pass filter between 3-70 Hz) later using software (e.g., LabChart Pro).
- Record a pre-injury baseline EEG for 30 minutes prior to disconnecting animals for carotid artery ligation procedure.
4. Left carotid artery ligation
- Anesthetize the pup (postnatal day 10) with 4-5% isoflurane in a downward flow hood and place them on specially arranged setup on a waterbath pad. Position the animal supine and secure the forelimbs with paper tape.
- Lower the flow of isoflurane to 2-3%. Pinch the tail for pain response and monitor breathing throughout procedure.
- Sterilize the incision area (between mandible and the clavicle) on the left side of the neck with betadine and alcohol (3 cycles of alternating iodine and 70% ethanol).
- Make an approximately 1 cm long incision on the left side of the neck using microscissors. Using a dissecting microscope, carefully retract the subcutaneous tissue and skin to expose the carotid artery. Take care to identify the vagus nerve (running lateral to the artery) and delicately separate and retract it from the artery.
- Thread a 5 cm long sterile silk suture under the artery using microforceps. Tie a double knotted suture around the artery to occlude flow.
- Cut the excess suture and close the exposed artery by pulling back the subcutaneous tissue and skin. Use vet bond to seal the incision.
- Place the animal back on continuous EEG monitoring in a chamber at room temperature, which is placed on a warming mattress. Take spot infrared temperature checks of pup core temperature to avoid opening the chamber. Allow the animal to recover for 1 h prior to hypoxia.
5. EEG and hypoxia
- Continuously monitor FiO2 (fraction of inspired oxygen) within the chamber via an oxygen monitor.
- Flush the chamber with 60 L/min of 100% N2 and 0.415 L/min for 100% O2. Once the oxygen saturation in the chamber reaches 12%, decrease the N2 flow to 10 L/min while keeping the O2 flow unchanged. With small adjustments, maintain the FiO2 at 8% for 45 min.
- After 45 min of hypoxia exposure, return FiO2 to 21%.
- Have pups recover in chamber and monitor on EEG for 2 h post-hypoxia.
- After completion of recording period, disconnect mice from EEG recording and return to the mother.
6. EEG analysis
- Analyze the EEG file with video in LabChart Pro. Have a blinded researcher mark the EEG for seizures and background patterns17. Seizures are defined as an electrographic event lasting greater than 10 seconds with high frequency rhythmic sharp wave discharges (≥3x baseline) with clear evolution17.
- Have a second blinded researcher review marked events at random for agreement.
- Review associated video for each marked electrographic event and analyze according to the neonatal rodent behavioral seizure score16. Briefly, this score ranges from 0-6 (immobility to severe tonic-clonic behavior). To further characterize seizure semiology, analyze behavior for laterality (multifocal/bilateral movements vs. focal/unilateral vs. mixed).
- Create a power spectrogram. Use a Fast Fourier Transform with a Cosine-Bell data window with a size of 1024 data points. Create a smooth x-axis in the spectrogram with the help of a window overlap of 87.5%. Express the power as µV218.
Subscription Required. Please recommend JoVE to your librarian.
Representative Results
Seizure semiology
Neonatal hypoxia-ischemia exposure results in both generalized and focal seizures in mice (Figure 1A-C). Video EEG recordings allow electrographic findings to be correlated to behavior on video. These behaviors were scored using a previously published neonatal rodent behavioral seizure score (BSS)16. In addition to BSS, we categorized events based on whether the behavior was focal/unilateral, bilateral, or mixed (Figure 1B).
In this model, mice generally exhibited 3 patterns of seizure semiology: 1) repetitive circling to the side of ligation with extension of contralateral extremities, 2) loss of posture with body flexion and tail curled to side of ligation, or 3) loss of posture with unilateral or bilateral paddling of extremities (varying severity and length). The majority of observed events involved focal/unilateral or mixed behaviors (Figure 1B). In addition, during the hypoxic period, a subset of mice exhibited non-convulsive seizure activity, where the pup was immobile with sustained seizure activity on EEG (Figure 1C).
Electrographic recordings
EEG recording was started 30 minutes prior to carotid ligation in order to obtain a pre-injury baseline. Baseline activity (Figure 1A and Figure 2A) was similar to previously described background in p10 mouse pups17. Following ligation, pups were immediately placed back on video EEG. During the period between ligation and commencement of hypoxia, a subset of mice exhibits convulsive seizures (Figure 1A-C).
Following hypoxia induction, background amplitude on EEG reduced (Figure 3B) and intermittently exhibited bursts of spike-wave discharges, followed by suppression (Figure 2A). Mice exhibit electrographic seizures, which emerge from a suppressed background as rhythmic spike-wave discharges and progress to become more complex and frequent, with polyspike waves (Figure 2B). During hypoxia, power spectrogram analysis was notable for asymmetries between the ischemic and contralateral hemisphere (Figure 3A,B). The ischemic hemisphere exhibited a burst suppression pattern and the contralateral hemisphere exhibited suppressed background (Figure 1A and Figure 3A,B). On average seizures begin 5.5±8.1 minutes after induction of hypoxia, with each event lasting 56±57 seconds. There was a 13% mortality rate during hypoxia (n=4/30), with all deaths following a convulsive (BSS=5-6) seizure.
During reoxygenation and recovery, a subset of mice continues to have seizures over the remainder of the recording period (2 h post-hypoxia). EEG background was suppressed compared to baseline following hypoxia (Figure 1A and Figure 3), with gradual recovery during the post-hypoxia recording period. Over the entire recording period, mice exhibited on average 9±5 seizure events, each lasted 54±57.7 s.
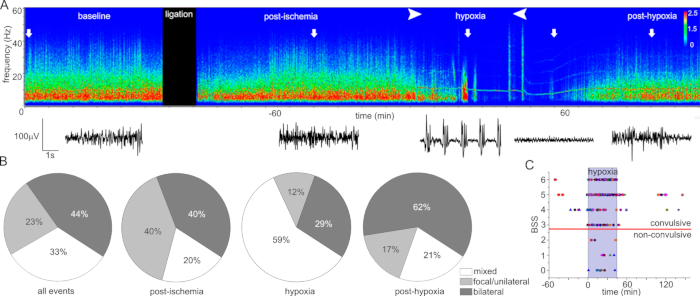
Figure 1: Seizure characteristics in p10 mice exposed to neonatal hypoxia–ischemia. (A) Representative power spectrogram from the ischemic parietal cortex electrode through the experimental timeline. (Amplitude color heat map scale x10–6). Arrows indicate the time that raw electroencephalogram tracings below the spectrogram represent. (B) Seizure behaviors for the entire experiment, postischemia/prehypoxia, during hypoxia, and posthypoxia. (C) Behavioral seizure score (BSS) and timing for all seizure events (n = 30 mice, each mouse has a unique symbol, each point is a discrete seizure event). 100% of mice seized during hypoxia (blue box; time = −60 minutes is the completion of carotid ligation, time=0 is the start of hypoxia). Thirteen percent died during hypoxia following a convulsive seizure (grade 5–6). This figure has been modified from Burnsed et al13. Please click here to view a larger version of this figure.

Figure 2: Characteristic electroencephalography (EEG) patterns during hypoxia ischemia. (A) EEG background from left to right: preinjury baseline, burst suppression during hypoxia, posthypoxia suppression. Recording from ipsilateral parietal cortex depth electrode. (B) Evolution of a seizure during hypoxia. Recording from ipsilateral hippocampal depth electrode. Shaded boxes (I-V) corresponded to expanded EEG excerpts on the right of (B). This figure has been modified from Burnsed et al13. Please click here to view a larger version of this figure.

Figure 3: Asymmetries in EEG background between ischemic and contralateral hemispheres. (A) Asymmetric power spectrogram in HI mice during hypoxia (45-minute period) in ischemic cortex (left) and contralateral cortex (right; amplitude scale x10–6). Burst suppression pattern and seizures in ischemic hemisphere, suppression in CL hemisphere. (B) Background suppression during hypoxia and reoxygenation in IL and CL hemispheres. All measurements of mean voltage taken from 10-second random excerpts of the encephalogram over the experimental time period (baseline, 30 minutes postligation, during hypoxia—15 minutes and 30 minutes after start, after reoxygenation—15 minutes and 60 minutes after start) were compared to baseline. Each animal’s baseline served as its own control, and data are reported as a percentage of baseline (n = 5 mice). Measurements were taken from cortical electrodes. This figure has been modified from Burnsed et al13. Please click here to view a larger version of this figure.
Subscription Required. Please recommend JoVE to your librarian.
Discussion
We have presented a model for continuous video-EEG monitoring in neonatal mice during hypoxic-ischemic seizures. Video analysis in conjunction with EEG allows characterization of seizure semiology. Analysis of EEG allows for extraction of power spectrograms and background amplitude analysis.
Correct and careful placement of electrodes is crucial in this protocol, as injury during electrode placement or inaccurate placement can significantly affect results. Assessment of normal baseline EEG activity prior to injury is paramount, as bleeding or injury during electrode placement, while rare, can happen. Secondly, in order to confirm correct electrode placement, brains can be sectioned and examined for electrode tracks in the proper placement. In addition, failure to return pups to the mother in groups (individually) may result in electrode headsets being damaged or pups being killed or neglected by the mother.
One limitation of this method is the limit of spatial localization of depth electrode recordings in a small neonatal brain. This restricts the ability to localize specific seizure foci on EEG recordings. Another limitation in this model of hypoxia ischemia is the variability in seizure burden. Variability in lesion size and behavioral deficits in this rodent model of hypoxia ischemia has been well described previously7,8,19. Not surprisingly, this variability exists in seizure burden (both length of seizure events and number of seizure events). However, consistently, 100% of pups in this model exhibit seizures during hypoxia. Lastly, the amount of time pups can be on EEG monitoring (away from the mother) is limited. Therefore, we are unable to characterize ongoing seizures with continuous EEG at later time points relative to the injury.
Although, we have used a hypoxia-ischemia seizure model in this manuscript, this method for continuous video-EEG monitoring in neonatal mouse pups could be easily applied to other disease/seizure models. Seizures in neonatal rodents are difficult to recognize based on behavior alone, making video-EEG monitoring important. Future investigations could use these techniques to analysis seizure burden and semiology in other neonatal seizure models or response to therapeutics and neuroprotective measures.
Subscription Required. Please recommend JoVE to your librarian.
Disclosures
None.
Acknowledgments
We acknowledge the following funding sources: NIH NINDS – K08NS101122 (JB), R01NS040337 (JK), R01NS044370 (JK), University of Virginia School of Medicine (JB).
Materials
| Name | Company | Catalog Number | Comments |
| SURGERY | |||
| Ball Point Applicator | Metrex Research | 8300-F | i-bond applicator |
| Cranioplast (Powder/Resin) | Coltene | H00383 | Perm Reline/Power |
| I-Bond | Kulzer GmbH, Germany | ||
| LOOK Silk Suture | Surgical Specialities Corporation | SP115 | LOOK SP115 Black Braided Silk Non absorbable surgical suture |
| RS-5168 Botvin Forceps | Roboz Surgical Instrument | RS5168 | Forcep for surgery/ligation |
| RS-5138 Graefe Forceps | Roboz Surgical Instrument | RS5138 | Forcep for surgery/ligation |
| UV light for I-Bond | Blast Lite By First Media | BL778 | UV ligth for I-bond |
| Vannas Microdissecting Scissor | Roboz Surgical Instrument | RS5618 | Scissor for ligation |
| Vet Bond | 3M Vetbond | 1469SB | Vet Glue |
| HYPOXIA | |||
| Hypoxidial | Starr Life Science | ||
| Oxygen sensor | Medical Products | MiniOxI- oxygen analyzer/sensor for hypoxia rig | |
| EEG RECORDING | |||
| Female receptacle connector 0.079" | Mill-Max Manufacturing Corp | 832-10-024-10-001000 | Ordered from Digikey |
| Grass Amplifier | Natus Neurology Incorporated | Grass Product | |
| LabChart Pro | ADI Instruments | Software to run the system | |
| Male Socket Connector 0.079" | Mill-Max Manufacturing Corp | 833-43-024-20-001000 | Ordered from Digikey |
| Operational Amplifier | Texas Instruments, Dallas, TX, USA | TLC2274CD | TLC2274 Quad Low-Noise Rail-to Rail Operational Amplifier |
| Operational Amplifier | Texas Instruments, Dallas, TX, USA | TLC2272ACDR | TLC2274 Quad Low-Noise Rail-to Rail Operational Amplifier |
| Stainless Steel wire | A-M Systems | 791400 | 0.005" Bare/0.008" Coated 100 ft |
| Ultra-Flexible Wire | McMaster-Carr | 9564T1 | 36 Gauze wire of various color |
References
- Vasudevan, C., Levene, M. Epidemiology and aetiology of neonatal seizures. Seminars in Fetal & Neonatal Medicine. , (2013).
- Volpe, J., et al.
- Shankaran, S., et al. Network EKSNNR. Childhood outcomes after hypothermia for neonatal encephalopathy. New England Journal of Medicine. 366 (22), 2085-2092 (2012).
- Pappas, A., et al. Cognitive outcomes after neonatal encephalopathy. Pediatrics. 135 (3), 624-634 (2015).
- van Schie, P. E., et al. Long-term motor and behavioral outcome after perinatal hypoxic-ischemic encephalopathy. European Journal of Paediatric Neurology. 19 (3), 354-359 (2015).
- Rensing, N., et al. Longitudinal analysis of developmental changes in electroencephalography patterns and sleep-wake states of the neonatal mouse. PLoS One. 13 (11), 1-17 (2018).
- Rice, J. E., Vannucci, R. C., Brierley, J. B. The influence of immaturity on hypoxic-ischemic brain damage in the rat. Annals of Neurology. 9 (2), 131-141 (1981).
- Burnsed, J. C., et al. Hypoxia-ischemia and therapeutic hypothermia in the neonatal mouse brain--a longitudinal study. PLoS One. 10 (3), 0118889 (2015).
- Semple, B. D., et al. Brain development in rodents and humans: Identifying benchmarks of maturation and vulnerability to injury across species. Progress in Neurobiology. , 1-16 (2013).
- Comi, A. M., et al. Gabapentin neuroprotection and seizure suppression in immature mouse brain ischemia. Pediatric Research. 64 (1), 81-85 (2008).
- Comi, A. M., et al. A new model of stroke and ischemic seizures in the immature mouse. Pediatric Neurology. 31 (4), 254-257 (2004).
- Kadam, S. D., White, A. M., Staley, K. J., Dudek, F. E. Continuous Electroencephalographic Monitoring with Radio-Telemetry in a Rat Model of Perinatal Hypoxia-Ischemia Reveals Progressive Post-Stroke Epilepsy. Journal of Neuroscience. 30 (1), 404-415 (2010).
- Burnsed, J., et al. Neuronal Circuit Activity during Neonatal Hypoxic - Ischemic Seizures in Mice. Annals of Neurology. 86, 927-938 (2019).
- Sampath, D., White, A. M., Raol, Y. H. Characterization of neonatal seizures in an animal model of hypoxic-ischemic encephalopathy. Epilepsia. 55 (7), 985-993 (2014).
- Sampath, D., Valdez, R., White, A. M., Raol, Y. H. Anticonvulsant effect of flupirtine in an animal model of neonatal hypoxic-ischemic encephalopathy. Neuropharmacology. 123, 126-135 (2017).
- Kang, S. K., et al. and sex-dependent susceptibility to phenobarbital-resistant neonatal seizures: role of chloride co-transporters. Frontiers in Cellular Neuroscience. 9, 1-16 (2015).
- Zanelli, S., Goodkin, H. P., Kowalski, S., Kapur, J. Impact of transient acute hypoxia on the developing mouse EEG. Neurobiology of Disease. 68, 37-46 (2014).
- Lewczuk, E., et al. EEG and behavior patterns during experimental status epilepticus. Epilepsia. 59 (2), 369-380 (2017).
- Wu, D., Martin, L. J., Northington, F. J., Zhang, J. Oscillating gradient diffusion MRI reveals unique microstructural information in normal and hypoxia-ischemia injured mouse brains. Magnetic Resonance in Medicine. 72 (5), 1366-1374 (2014).
