Induction and Assessment of Exertional Skeletal Muscle Damage in Humans
Summary
This article describes a safe and reliable method to induce and quantify exertional skeletal muscle damage in human subjects.
Abstract
Contraction-induced muscle damage via voluntary eccentric (lengthening) contractions offers an excellent model for studying muscle adaptation and recovery in humans. Herein we discuss the design of an eccentric exercise protocol to induce damage in the quadriceps muscles, marked by changes in strength, soreness, and plasma creatine kinase levels. This method is simple, ethical, and widely applicable since it is performed in human participants and eliminates the interspecies translation of the results. Subjects perform 300 maximal eccentric contractions of the knee extensor muscles at a speed of 120°/sec on an isokinetic dynamometer. The extent of the damage is measurable using relatively non-invasive isokinetic and isometric measures of strength loss, soreness, and plasma creatine kinase levels over several days following the exercise. Therefore, its application can be directed to specific populations in an attempt to identify mechanisms for muscle adaptation and regeneration.
Introduction
The overall goal of this procedure is to induce exertional damage to the quadriceps femoris muscles using voluntary lengthening (eccentric) contractions in human subjects.
Contraction-induced skeletal muscle damage is a common consequence of exercise that is marked by delayed onset muscle soreness1, transient strength loss, and elevated muscle-specific enzymes in the blood2. Exertional muscle damage is most pronounced following exercise to which the subject is unaccustomed, particularly when eccentric contractions are involved3. Exertional muscle damage is typically benign. Soreness subsides, and both serum proteins and strength typically return to pre-damage levels within a few days to weeks after the damaging insult. In extreme cases, exertional muscle damage can lead to a life-threatening syndrome know as rhabdomyolysis. However, exertional muscle damage is usually insufficient to cause clinical rhabdomyolysis in healthy individuals4 in the absence of compounding factors including heat stress, dehydration5, infection6 or rare genetic predispositions7.
Contraction-induced muscle damage is typically less severe than toxin-induced or freezing-induced injury, methods often used in rodent studies8,9. Yet, contraction-induced injury provides a useful method to study the muscle damage response with notable advantages. First, it is a safe and ethical method for use with human subjects1-3. Thus, interspecies translation of the results is not needed as data can be obtained directly from human subjects. Moreover, translating data obtained from rodent studies is very difficult given that the severity of injury seen in the rodent injury models exceeds the level of damage that would be ethical to induce in human subjects. Second, contraction-induced damage is commonly experienced and a natural process of exercise. Therefore, this mode of damage induction is useful for studying muscle damage in the context of exercise, adaptation to exercise as well as overt muscle injury. Here we describe a safe and reliable method to induce and evaluate skeletal muscle damage using lengthening contractions in humans.
Protocol
The following procedures are in accordance with the standards of the Brigham Young University Institutional review board (IRB).
1. Prepare the Contraction Protocols
NOTE: The following protocol instructions are based on the Biodex Advantage software. Navigating the software and operating the dynamometer will be different if different systems are used.
- Isokinetic Strength Test Protocol
- To make the isokinetic protocol, open dynamometer control software on the computer and select the "Protocol" tab and then select the "Record" tab on the toolbar on the top of the screen. Select "New Protocol" from the dropdown list.
- In the "Study Type" box, select the "Test" option.
- Select the following parameters from the dropdown menus: Under the "Mode" menu select Isokinetic. Under the "Joint" menu select knee. Under the "Pattern" menu select extension/flexion. Select concentric contractions for both extension and flexion movements. Select "reps" under the "End By" dropdown menu.
- On the "Unilateral" tab program 1 set of 3 repetitions at a speed of 60°/sec for both the away and toward contractions. To do this, enter "1" into the "# sets" field and type "3" in the "End By Reps" row. Then type 60 in both the "Speed Away" and "Speed Toward" rows.
- Use 90° as the anatomical reference point and set range of motion limits to approximately 10° away and 110° towards (0° = full extension, 135° = full flexion).To do this, select the "set ROM" button on the left side of the screen. Calibrate the lever arm so that 90° is parallel to the floor (as indicated using the lever arm angle indicator provided on the computer screen). Then using 90° as the anatomical reference point, set the range of motion limits to approximately 10° away and 110° towards (0° = full extension, 135° = full flexion).
NOTE: The joint angle settings given here are preferred, however these settings should be modified on a case-by-case basis especially when working with subjects with a fixed flexion deformity or other limitation. - Name the protocol in the "Description" field on the bottom left of the screen and select the save button on the top menu bar.
- Isometric Strength Test Protocol
- Repeat steps 1.1.1 to begin making the isometric protocol.
- Select the "Test" option from the "Study Type" box.
- Select the following parameters from the dropdown menus: Under the "Mode" menu select "isometric". Under the "Joint" menu select "knee". Under the "Pattern" menu select "extension/flexion". Under the "Contraction Direction" menu select "away". In the "End By" menu select "reps".
- Program a test with 1 set of 3 isometric contractions lasting 5 sec each at a joint angle of 70°. To do this, type "1" into the "Positions" field on the "Unilateral" tab. Under the position #1 column, type "3"in the "End by Reps" row. In the row labeled "Angle" select "70".
- Select 90° as the anatomical reference point and an away limit to 70°.
- Name the protocol in the "Description" field on the bottom left of the screen and select the save button on the top menu bar.
- Muscle Damaging Eccentric Exercise Protocol
- To make the eccentric exercise protocol, open dynamometer control software on the computer and select the "Protocol" tab. Then select the "Record" tab on the toolbar on the top of the screen. Now click on "New Protocol" from the dropdown list.
- Select the "Exercise" option from the "Study Type" box.
- Select the following parameters from the dropdown menus: Under the "Mode" menu select "isokinetic". Under the "Joint" menu select "knee". Under the "Pattern" menu select "Extension/Flexion". Under the "Contraction" menu select "Con/ECC".
- On the "Unilateral" tab, program 10 sets of 10 repetitions at speeds of 180°/sec away and 120°/sec towards with 60 sec rest between sets.
- Type "10" into the "# Sets" field.
- In the first column (labeled #1), type "10" in the row labeled "End by Reps". Then type "180" in the next row labeled "Speed Away". In the next row labeled "Speed Toward", type "120". In the row labeled "Torque", type 200 to 600 depending on the anticipated strength of the subject.
- Repeat step 1.3.4.2 for sets #2 through #10.
- Type 60 in the "Rest Time in secs" field.
- Type 90° into the "Anatomical Reference" field.
- Select the "Set ROM" button on the left side of the screen and set range of motion limits to 40° away and 110° towards (0° = full extension, 135° = full flexion). These settings provide the range of motion through which the subject must provide resistance against the arm of the dynamometer. As a safety precaution, the dynamometer will stop moving if the subject stops providing resistance within this specified range of motion.
- To set the range of motion, select the "set ROM" button on the left side of the screen. Calibrate the lever arm so that 90° is parallel to the floor (as indicated using the lever arm angle indicator provided on the computer screen). Then using 90° as the anatomical reference point, set the range of motion limits to 40° away and 110° towards (0° = full extension, 135° = full flexion).
NOTE: These joint angle settings are suggestions for a typical healthy subject. These should be modified to fit the abilities from one individual to another.
- To set the range of motion, select the "set ROM" button on the left side of the screen. Calibrate the lever arm so that 90° is parallel to the floor (as indicated using the lever arm angle indicator provided on the computer screen). Then using 90° as the anatomical reference point, set the range of motion limits to 40° away and 110° towards (0° = full extension, 135° = full flexion).
- Name the protocol in the "Description" field and select the "Save" button at the top tool bar.
2. Baseline Measurements
- Soreness Measurements
- Make a visual analog scale by drawing a 100 mm line horizontally across a page.
- On the left-hand side of the line indicate "No soreness" and on the right-hand side of the line indicate "Extreme soreness" (Figure 1). This method is commonly used to assess delayed-onset muscle soreness1,10,11.
- Instruct the subject to do two body-weight squats. Perform both squats with arms held straight out in front of the shoulders and feet shoulder-width apart. Proper depth is reached when the upper legs are parallel to the floor before returning to the start position.
- Ask the subject to indicate the intensity of the soreness he or she felt in the quadriceps femoris muscles during the squats by drawing a vertical line at the appropriate spot on the visual analog scale.
- Quantify the subject's level of soreness by measuring the distance in millimeters from the no-soreness end of the visual analog scale to subject's mark.
- Serum Creatine Kinase
CAUTION: Wear protective gloves before handling blood and dispose of needles immediately after use in a sharps container as per hospital or university policy.- Follow standardized phlebotomy procedures to withdraw blood from the antecubital region of the subject's arm under fasting conditions to obtain 5 to 6 ml of blood12.
- Centrifuge the blood sample at 15 x g for 15 min at 3 °C to separate serum from blood cells.
- Using a transfer pipette, transfer the serum sample into a microcentrifuge tube labeled appropriately for subject and time point.
- Store the sample at -80 °C for later use.
- Assay the serum samples for creatine kinase activity using a commercially available kit according to manufacturer's protocol. Alternatively, the serum samples can be transported to a local medical diagnostic laboratory for analysis.
- Subject Preparation
- Forty-eight hours prior to the subject's visit, instruct them to avoid strenuous or unaccustomed exercise, non-steroidal anti-inflammatory drugs and alcohol.
- When the subject arrives, collect weight, height, sex, and leg dominance information prior to setup. Leg dominance can be determined by asking the subject with which leg they would choose to kick a ball.
- Have the subject warm up at 50 to 150 W for 10 min on a bicycle ergometer before performing the strength tests.
- After the warm-up ask the subject to sit in the chair of the dynamometer. Adjust the tilt, height, depth, recline, and rotation of the seat and shaft arm to fit the subject. Use the lateral femoral condyle as a reference and align rotational axis of the knee with that of the dynamometer shaft arm. Adjust the shaft arm length so that it is just proximal to the medial malleolus, and secure with strap. Subject should be able to plantar flex comfortably with full range of motion.
- Leave sufficient space (25 mm) between the front edge of the seat and the back of the leg to allow maximal flexion of the knee joint without pinching or discomfort.
- Stabilize subject with shoulder, hip, ankle and thigh straps. To isolate the knee extensors and avoid ancillary muscle involvement, it is essential that the subject be securely stabilized.
- Have the subject perform 3-5 practice extension/flexion maneuvers of the knee, monitor range of motion and signs of discomfort that may exist prior to beginning the contraction protocol, and adjust as needed.
- Now that the adjustable components of the dynamometer are properly fitted to the subject, record the seat position settings and shaft arm position for repeatable setup on subsequent visits.
NOTE: It is important that the subject is safe and comfortable. The dynamometer is equipped with an emergency stop button for both the subject and operator in the case of an emergency.
- Force Measurement
- After the subject is properly oriented in the seat and the isometric strength test protocol is loaded, instruct the subject on how to perform the test.
- Tell the subject that he or she will be contracting against the lever arm that will stay stationary. Tell the subject to follow the prompts of the computer screen doing 3 contractions lasting 5 sec each.
- Tell the subject to maintain maximal effort for each contraction. Tell the subject to breathe during the contractions. Ask the subject to cross their arms across the chest during the test.
- Start the isometric protocol and allow the subject to practice the test with submaximal effort. This practice trial will familiarize the subject to the test as well as provide a test-specific warm-up. Allow the subject to practice the test 2 to 3 times.
- Once the subject is ready, start the test and verbally encourage the subject to provide maximal effort for each contraction.
- Record torque, power, and work. The software also calculates the coefficient of variance (a statistical representation of test validity based on reproducibility of performance, lower values indicate higher reproducibility). If the coefficient of variance exceeds 15%, repeat the test. Repeat the test up to 4 times. If the subject is unable to produce a coefficient of variance less than 15% after 4 attempts use the data from the set that yielded the lowest coefficient of variance value.
- Allow the subject two to three minutes to rest, and then load the isokinetic protocol to obtain isokinetic strength data.
- After the subject is secured in the seat, instruct on how to perform the isokinetic test.
- Tell the subject that they will be doing three extension and flexion contractions against the lever arm that will move at a fixed rate. Tell the subject the goal is to contract as forcefully as possible throughout the entire range of motion for each contraction.
- Tell them that the lever arm will stop when they reach the end of the range of motion. Ask the subject to cross his arms across the chest during the test. Remind the subject not to hold their breath during the contractions
NOTE: While the data gathered from the flexion component of the contraction may not be of interest to the researcher, subjects who provide maximal effort for both the flexion and extension maneuvers tend to yield better force consistency during the extension maneuver.
- Start the test and verbally encourage the subject to provide maximal effort.
- Record torque, power, and work. The software also calculates the coefficient of variance (a statistical representation of test validity based on reproducibility of performance, lower values indicate higher reproducibility). If the coefficient of variance exceeds 15%, repeat the test.
- Repeat the test up to 4 times. If the subject is unable to produce a coefficient of variance less than 15% after 4 attempts, use the data from the set that yielded the lowest coefficient of variance value.
- After the subject is properly oriented in the seat and the isometric strength test protocol is loaded, instruct the subject on how to perform the test.
3. Damage Induction
- One to three days after the baseline measurements of Part 2, have the subject return to the lab for the damage induction portion of the protocol
- Have the subject warm-up on a cycle ergometer for 10 min at 50 to 150 W.
- After the warm-up, orient and secure the subject in the dynamometer using the adjustment settings recorded in step 2.3.7, load the muscle damaging eccentric exercise protocol and instruct the subject on how to properly perform the exercise.
- Tell the subject that they will contract against the lever arm to initiate the movement of the shaft arm for each contraction. Tell the subject that as the shaft arm moves toward them at a fixed rate, their goal is to contract against it as forcefully as possible.
- Allow the subject to grasp the handgrips located on either side of the seat.
- Tell the subject to breathe during the contractions; exhale during the eccentric phase.
- When the subject is ready, start the first set of contractions by pushing the start button on the screen.
- Verbally encourage the subject to maintain maximal effort for each contraction.
- Follow the prompts on the screen that will guide the subject through 10 sets of 10 repetitions with a 1 min rest period between sets.
- Once 10 sets are completed allow the subject 1 to 5 min to rest before repeating the protocol.
NOTE: The maximum number of sets available under the eccentric protocol is 10 however this may vary depending on the dynamometer and software used. The rest provides time for the operator to reload the protocol if necessary. - Repeat the procedure two more times for a total of 300 predominantly eccentric contractions.
4. Muscle Damage Assessment
- Repeat both Isokinetic and isometric strength tests as described in 2.4 immediately after the damaging exercise and at 24, 48, 72, and 96 hr after.
- Repeat the soreness measurement as described in part 2.1 at 24, 48, 72, and 96 hr after damaging exercise. Be sure to use a new visual analog scale for each assessment so that the subject cannot see their previous responses.
- Repeat the blood draw as described in part 2.2 for the creatine kinase assay at 48 and 120 hr after damaging exercise, or at time points dictated by the experimental protocol.
- Plot the creatine kinase, strength and soreness data on the y-axis of a graph against time on the x-axis.
- Observe how these variables deviate from and return toward baseline values in the days following exercise, indicating damage and repair, respectively.
Representative Results
Using the methods presented here, baseline soreness, serum creatine kinase activity, and strength (isometric and isokinetic) measurements were taken in 7 untrained young men. The following day, the subjects underwent the muscle damaging eccentric contraction protocol described above. To provide indices of muscle damage, follow up assessments of strength, soreness and serum creatine kinase activity were made. Strength was measured immediately after as well as 24, 48, 72, and 96 hr after exercise. Soreness was measured 24, 48, 72, and 96 hr after exercise. Serum creatine kinase was measured at 48 and 120 hr following exercise. These data were analyzed using a one-way repeated measures analysis of variance with a Dunnett's multiple comparison tests to compare post-exercise values to the pre-exercise value. Compared to pre-exercise, isometric and isokinetic force was decreased out to 24 and 48 hr post-exercise, respectively, and returned similar to pre-exercise values thereafter (Figure 2). Soreness was significantly increased at 24, 48, and 72 hr after exercise (Figure 3). Serum creatine kinase was significantly elevated 48 hr after exercise (Figure 4). Figure 5 shows an atypical isometric force curve in the days following damaging exercise.

Figure 1: The visual analog scale used to quantify muscle soreness of the quadriceps femoris muscles. Subjects are instructed to do two bodyweight squats and then indicate on the line the degree of soreness they felt in the quadriceps muscles during the squat maneuver. The researcher quantifies this by measuring the distance of the mark in mm from the no-soreness end of the scale. Please click here to view a larger version of this figure.
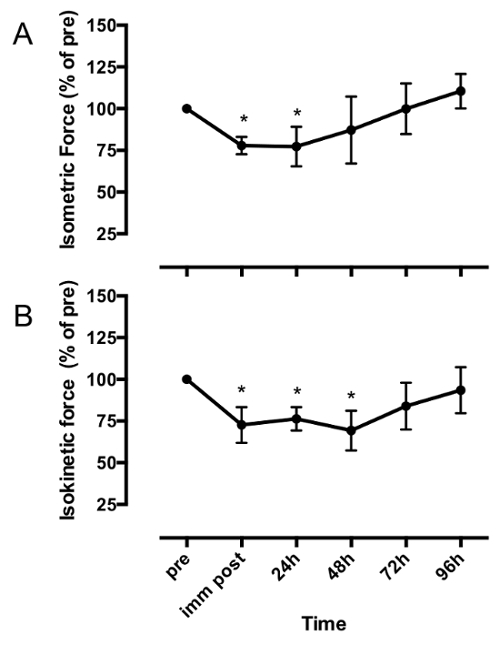
Figure 2: Isometric force (A) and 60o/s isokinetic force (B) of the knee extensor muscles one day before (pre), immediately after (imm post), 24, 48, 72, and 96 hr after a bout of 300 maximal effort lengthening contractions. Data are expressed as a percent of the pre-exercise force value (mean ± SD). Data were analyzed with a one-way repeated measures analysis of variance with a Dunnett's test for multiple comparisons. * indicates significant difference from pre (p < 0.05). This figure is adapted from reference3. Please click here to view a larger version of this figure.

Figure 3: The soreness response curve one day before exercise (pre) as well as at 24, 48, 72, and 96 hr following 300 maximal-effort lengthening contractions. The data are expressed on the log10 scale (mean ± SD). * indicates significant difference from pre exercise (p < 0.05). This figure is adapted from reference3. Please click here to view a larger version of this figure.

Figure 4: Serum creatine kinase (CK) activity (mean ± SD) 24 hours before (pre), 48 and 120 hr after 300 maximal-effort lengthening contractions (LC). Data are presented as the percentage of pre-exercise values on the log10 scale. * Indicates significant difference from pre (p < 0.05), n.s. indicates no significant difference. Please click here to view a larger version of this figure.

Figure 5: Isometric force of the knee extensor muscles of one subject who showed an atypical response. Force measurements immediately after (imm post) 24, 48, 72, and 96 hr after a bout of 300 maximal effort lengthening contractions were not reduced compared to the pre exercise (pre) value in this subject. Please click here to view a larger version of this figure.
Discussion
Several steps are critical to obtaining the desired results of this protocol. First, subjects must be adequately familiarized to the contraction protocols, particularly the force measurements. Be sure that the subject understands exactly what they are expected to do and give them an opportunity to practice the strength tests prior to data collection. Subjects who are not adequately familiarized with these procedures may show a learning curve over the days following the damage induction. This can be a confounding variable rendering the strength measurements invalid. Figure 5 shows data from an individual who may have not been properly familiarized. This subject showed increasing strength due, perhaps, to learning over the course of the experiment despite the damaging exercise. Second, the selection of the subject population may also be critical to this protocol. Exertional muscle damage may vary greatly from subject to subject depending on many factors, including the trained status of the individual. Individuals accustomed to eccentric exercise will show much less damage compared to unaccustomed individuals. This may be an important consideration when selecting a subject population. If a researcher is interested in observing a large damage response, a population unaccustomed to eccentric exercise will be most likely to provide this outcome. Finally, it is critical that the subject is consistently positioned on the dynamometer over the repeated visits. The researcher should record the position settings for each adjustable component of the dynamometer for each subject and reposition it accordingly for each follow-up test. This will minimize variability due to postural differences.
Many different dynameters are available. While the methods provided here are specific to the Biodex dynamometer and control software, these methods can be adapted for use with other dynamometers after accounting for operating differences. The use of the dynamometer as presented here provides advantages over some other methods used to induce muscle damage in humans. These advantages include accurately quantifying the total work done during the exercise, controlling angular velocity, and accurately measuring strength and strength loss. However, other methods of damage induction can be used in the event that a dynamometer is not available or not preferred. Hubal and co-workers13 used a repeated chair sit and rise method to effectively induced muscle damage. In this study, subjects performed lengthening contractions by lowering into a chair. Stupka and co-workers14 used traditional knee extensor exercise during which subjects performed the lengthening component of the contraction at 120% of concentric one repetition maximum. Downhill running is also an effective stimulus to cause muscle damage15,16. These other methods of damage induction may be preferred if the researcher is interested in observing damage from a more real-world or sport-specific stimulus or from a closed kinetic chain movement. Another modification to this protocol that the researcher may consider is the frequency of blood sampling for creatine kinase measurement. To get the most informative picture of serum creatine kinase post-exercise, the researcher may choose to take blood samples every 24 hr for five to six days after damage. This will ensure that the peak serum creatine kinase values are not missed. Also this will provide better information as to the nature of the changes in serum creatine kinase, such as whether the curve follows a mono or biphasic shape.
One limitation of this protocol is that the strength loss, serum creatine kinase, and soreness, are indirect markers of damage. While direct evidence of damage can be observed by obtaining a muscle sample and using electron microscopy, other histological methods used in rodent studies do not detect voluntary contraction-induced damage in human muscle17,18. Considering the limited methods capable of directly detecting muscle damage in the context of voluntary contraction-induced damage in humans, indirect markers of damage are among the best options10.
Aspects of both data collection and analysis may require troubleshooting. During the muscle damaging protocol, the subject must trigger the movement of the shaft arm for each eccentric contraction. The subject does this by contracting against the stationary arm in an extended knee position until a threshold force value is met which triggers the shaft movement and the eccentric contraction. The threshold force value is 10% of the torque value programed into the contraction protocol (step 1.3.4.2). Subjects may have difficulty meeting the threshold force in the extended knee start position, especially after several sets have been completed. The researcher can help the subject reach the threshold to initiate the contractions by pulling on the shaft arm. Alternatively, the torque value programed into each contraction of the protocol (1.3.4.2) can be reduced so that the threshold is lower. However, the torque value must not be set too low because if the subject exceeds the torque value the shaft arm will stop and the contraction will be interrupted. The nature of the creatine kinase and soreness data may also provide some trouble for the investigator. These data sets are often not normally distributed. Both variables tend to show non-homogeneity of variance such that increased variability occurs with higher mean values. Due to the nature of these variables, a log transformation is often appropriate to normalize the distributions and homogenize the variance prior to statistical analysis. Alternatively, non-parametric tests may be used.
The exercise-induced muscle damage protocol described in this paper may have broad applications. The primary strength of using the protocol is the potential to study the cellular and molecular processes that govern muscle repair, regeneration, and adaptation directly in human subjects. Furthermore, delayed onset muscle soreness and temporary strength losses are often undesired consequences of strenuous, or novel exercise. Using an exercise-based damage protocol such as the one described here, researchers are provided a validated model can test the effectiveness of nutritional, nutraceutical, or pharmacological interventions or other treatments meant to protect against delayed onset muscle soreness following exercise.
In conclusion, this manuscript describes a safe and reliable method to cause and quantify contraction-induced skeletal muscle damage in humans. It uses eccentric contractions of the knee extensors that are controlled by a dynamometer to induce damage. Muscle damage is assessed noninvasively with delayed onset muscle soreness, serum creatine kinase and strength loss. While the protocol is written for a specific dynamometer for damage induction and force measurements, this protocol can be adapted for use with other dynamometers as well as other modes of contraction induced damage all together.
Divulgazioni
The authors have nothing to disclose.
Acknowledgements
The authors have no acknowledgements.
Materials
| Biodex Dynomometer | Biodex Medical Systems | 850-000 | Other models are available and should produce similar results |
| Creatine Kinase kit | Sigma-Aldrich | MAK116 | |
| Serum Vacutainers | BD Bioscience | 367812 | |
| Winged safety push button blood collection set | BD Bioscience | 367338 | |
| Cryogenic vials | Sigma-Aldrich | V5007 | We use the 2mL vials to store serum aliquots |
Riferimenti
- Deyhle, M. R., et al. Skeletal Muscle Inflammation Following Repeated Bouts of Lengthening Contractions in Humans. Front. Physiol. 6, 424 (2015).
- Hyldahl, R. D., et al. Extracellular matrix remodeling and its contribution to protective adaptation following lengthening contractions in human muscle. FASEB J. 29 (7), 2894-2904 (2015).
- Hyldahl, R. D., Olson, T., Welling, T., Groscost, L., Parcell, A. C. Satellite cell activity is differentially affected by contraction mode in human muscle following a work-matched bout of exercise. Front. Physiol. 5, 485 (2014).
- Clarkson, P. M., Kearns, A. K., Rouzier, P., Rubin, R., Thompson, P. D. Serum creatine kinase levels and renal function measures in exertional muscle damage. Med. Sci. Sports Exerc. 38 (4), 623-627 (2006).
- Clarkson, P. M. Exertional rhabdomyolysis and acute renal failure in marathon runners. Sports Med. 37 (4-5), 361-363 (2007).
- Seedat, Y. K., Aboo, N., Naicker, S., Parsoo, I. Acute renal failure in the "Comrades Marathon" runners. Ren. Fail. 11 (4), 209-212 (1989).
- Landau, M. E., Kenney, K., Deuster, P., Campbell, W. Exertional rhabdomyolysis: a clinical review with a focus on genetic influences. J. Clin. Neuromuscul. Dis. 13 (3), 122-136 (2012).
- Warren, G. L., et al. Role of CC chemokines in skeletal muscle functional restoration after injury. Am. J. Physiol. Cell Physiol. 286 (5), C1031-C1036 (2004).
- Zhang, J., et al. CD8 T cells are involved in skeletal muscle regeneration through facilitating MCP-1 secretion and Gr1(high) macrophage infiltration. J. Immunol. 193 (10), 5149-5160 (2014).
- Cermak, N. M., Noseworthy, M. D., Bourgeois, J. M., Tarnopolsky, M. A., Gibala, M. J. Diffusion tensor MRI to assess skeletal muscle disruption following eccentric exercise. Muscle Nerve. 46 (1), 42-50 (2012).
- Chen, Y. W., Hubal, M. J., Hoffman, E. P., Thompson, P. D., Clarkson, P. M. Molecular responses of human muscle to eccentric exercise. J. Appl. Physiol. 95 (6), 2485-2494 (2003).
- Stasinger, S. K., Di Lorenzo, M. S. . Phlebotomy Textbook. , 188-203 (2011).
- Hubal, M. J., Chen, T. C., Thompson, P. D., Clarkson, P. M. Inflammatory gene changes associated with the repeated-bout effect. Am. J. Physiol. Regul. Integr. Comp. Physiol. 294 (5), R1628-R1637 (2008).
- Stupka, N., Tarnopolsky, M. A., Yardley, N. J., Phillips, S. M. Cellular adaptation to repeated eccentric exercise-induced muscle damage. J. Appl. Physiol. 91 (4), 1669-1678 (2001).
- Smith, L. L., et al. Changes in serum cytokines after repeated bouts of downhill running. Appl. Physiol. Nutr. Metab. 32 (2), 233-240 (2007).
- Marqueste, T., Giannesini, B., Fur, Y. L., Cozzone, P. J., Bendahan, D. Comparative MRI analysis of T2 changes associated with single and repeated bouts of downhill running leading to eccentric-induced muscle damage. J. Appl. Physiol. 105 (1), 299-307 (2008).
- Crameri, R. M., et al. Myofibre damage in human skeletal muscle: effects of electrical stimulation versus voluntary contraction. J. Physiol. 583 (Pt 1), 365-380 (2007).
- Yu, J. G., Malm, C., Thornell, L. E. Eccentric contractions leading to DOMS do not cause loss of desmin nor fibre necrosis in human muscle. Histochem. Cell Biol. 118 (1), 29-34 (2002).
- Jamurtas, A. Z., et al. Comparison between leg and arm eccentric exercises of the same relative intensity on indices of muscle damage. Eur. J. Appl. Physiol. 95 (2-3), 179-185 (2005).
