For this study, the ex vivo technique was used in a correlative analysis of therapeutic sensitivity/resistance of a heat shock protein 90 inhibitor (Hsp90i). In a preclinical assessment of this Hsp90i, the breast cancer primary tumor, an ER+ invasive ductal carcinoma (IDC), and associated lymph node metastasis were analyzed ex vivo for treatment response (Figure 1). Multiple 200 μm serial sections were treated with vehicle only and increasing doses (0.25, 0.50, 1.0 and 2.5 μM) of the Hsp90i. The data in Figure 1 represents formalin-fixed, paraffin-embedded (FFPE) and hematoxylin & eosin (H&E) stained sections following a 48 hr treatment period. The control (vehicle only) treated section shows viable IDC nests whereas the 2.5 μM treated tissue section resulted in a 40% induction of apoptosis as seen by nuclear morphological changes (i.e., pyknotic nuclei/apoptotic debris) (Figure 1A). Apoptosis was further confirmed in the primary tumor by terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) analysis (data not shown). IC50 is calculated from response data by graphing percent apoptosis versus concentration of the drug. Significantly, the chaperone, Hsp90 plays a key role in protein stabilization and homeostasis of critical signaling pathways of both normal and cancer cells 10. The ability to target Hsp90 in cancer relies on the finding that malignant cells heavily depend on the chaperoning function of Hsp90, especially in an effort to overcome stressed states of inhospitable environments encountered during metastatic progression. In essence, cancer cells become highly dependent on Hsp90 function resulting in a targetable selective pool of ‘oncogenic’ Hsp90 11. In the insert, Figure 1A, adjacent benign lobule with associated acini and duct remains unaltered in the same 2.5 μM Hsp90i-treated section. To our knowledge, this is the first time this Hsp90 cancer-specificity is visually captured in Hsp90i response-assessment of primary tumors and associated metastases. This finding of unaltered benign/normal cells as seen in adjacent benign lobules of IDC (Figure 1A) as well as vessels within the surrounding benign breast parenchyma of the primary tumor and associated lymph node metastases (data not shown) has been recapitulated in several different tumor types (e.g., breast, gastric and lymphoma metastases).
An accompanying lymph node metastasis of this primary tumor showed a complete response only in the IDC nests that were loosely associated (Figure 1B). IDC nests that formed tight spheroids, however, remained viable as confirmed by TUNEL (Figure 1C). Additional analysis of the viable IDC spheroids by immunofluorescence revealed a persistent or re-expression of the cell-cell adhesion molecule, E-cadherin (Figure 1C). This finding is consistent with persistent, over-expression of E-cadherin adding to the metastatic potential or metastatic efficiency as reflected in the highly malignant, lethal inflammatory breast cancer 12, 13. Although interesting, this finding is beyond the scope of this paper. However, it is significant to note that these lymph node (LN) IDC spheroids were maintained in culture for a period of 2 weeks and thus lends credence to the strength of using the ex vivo technique to study both sensitivity/resistance in preclinical drug development.
The ex vivo technique has also been employed in a clinical study on core needle biopsies (CNBs) for evidence of target inhibition in tumors16,17. Patients who consent, have a pre-treatment core needle biopsy (CNB) procedure performed (Figure 2). Comparable to the preclinical assessment of primary tumors, the ex vivo technique is used to determine sensitivity or response in the CNB of accessible metastases. Multiple 200 μm serial sections of the CNB were treated with vehicle only and increasing doses (0.25, 0.50, 1.0 and 2.5 μM) of the Hsp90i. The number of Hsp90i doses used in ex vivo assessment is dictated by the size of CNB. However, every effort is made to use the spectrum of doses suggested above. Like the preclinical ex vivo assessment, response can be evaluated and later compared to the actual in patient response (i.e., correlative analyses; Figure 2) as determined by post-treatment CNB pharmacokinetic (PK), i.e., drug retention as measured via liquid chromatography tandem mass spectrometry (LC-MS/MS) analyses as well as in patient PET imaging (Figure 2)16,17. To date, analyses using the ex vivo technique in this clinical study has been performed on multiple tumor types (e.g., breast, marginal zone lymphoma, mantle cell lymphoma, metastatic paraganglioma, cervix and ovarian cancers)16, 17. Full correlative analysis implementing the ex vivo technique further exemplifies the utility of this technique in clinical drug development.
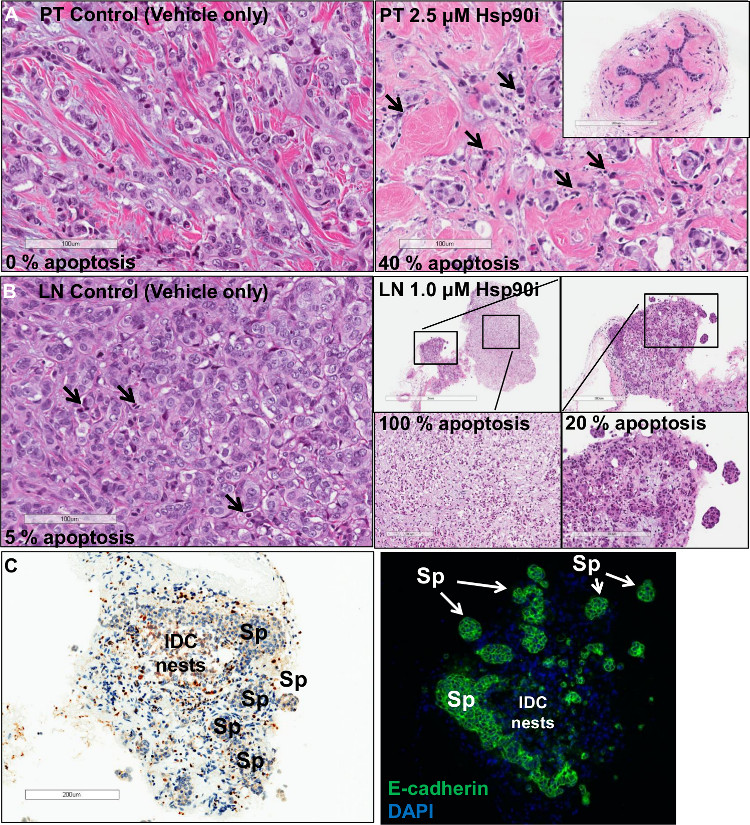
Figure 1. Ex vivo response analysis of an ER+ breast cancer. (A, Left panel) displays viable nests of invasive ductal carcinoma (IDC) (Hematoxylin and eosin stained; scale bar 100 μm). Upon treatment (A, right panel) with 2.5 μM of Hsp90i there is an induction of ~40% apoptotic response (pyknotic nuclei/apoptotic debris; arrows) (Hematoxylin and eosin stained; scale bar 100 μm). Benign lobules (A, insert) remain unaltered following treatment (Hematoxylin and eosin stained; scale bar 200 μm). The control of an associated lymph node (LN) (B, left panel) displays a small level of apoptosis (Hematoxylin and eosin stained; scale bar 100 μm), whereas the treated section (B, right panels) show an area of metastatic IDC nests with complete response (Hematoxylin and eosin stained; scale bar, clockwise 2 mm, 300 μm, 200 μm and 200 μm). However, tight IDC spheroids (Spheroids; Sp) from the same section (C, left panel) show little, if any, apoptosis as shown by TUNEL analysis remaining viable with a concomitant (scale bar 200 μm) (C, right panel) over-expression of E-cadherin (magnification 100X). Please click here to view a larger version of this figure.
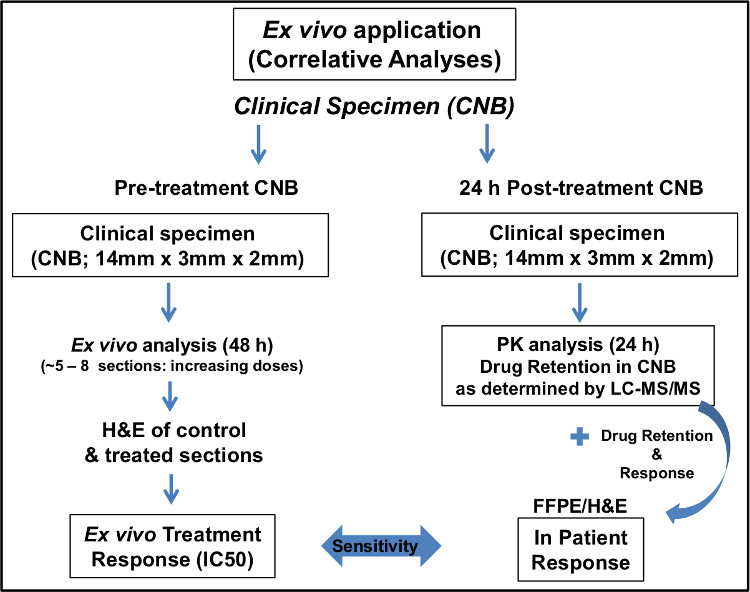
Figure 2. Schematic of implementation of ex vivo technique in a clinical study. Please click here to view a larger version of this figure.
