The methodology proposed here is commonly used in living patients and consideration of its novelty to deceased individuals should be noted. Figure 6 and Figure 8 present the results of an AP lumbar spine and left hip scan, respectively. The individual assessed in these scans is a deceased white, female, 31 years of age that is housed at the Forensic Analysis Laboratory of North Carolina State University. This individual had a total BMD score of 0.944 g/cm2 with a corresponding t-score (-0.9) for the ancestry and sex-matched reference population. According to the WHO classification, her BMD score is clinically normal and not below the –2 t-score that suggests a BMD consistent with osteoporosis/increased fracture risk8,83. The results presented are from three forensic cases where BMD scores were used to assess different etiologies in each individual set of remains. The methodology proposed has not been systematically assessed in skeletal remains, but in combination with other methods can aid the investigator during their assessment. Case study 1 illustrates its use in adults whereby perimortem, longitudinal cracking is evident in the long bones. BMD scores were used to assess whether this cracking was due to fracture risk during life or postmortem processes where color change comparison was not applicable. Case study 2 illustrates its use in juvenile remains when long-term abuse and neglect are suspected. Case study 3 illustrates the method's use in infant deaths when fatal starvation is suspected.
In Case Study 1, this individual was a 40-year-old male exhibiting a rare fracture series that includes longitudinal fractures of both anterior surfaces of the femur and tibia that completely penetrated the cortical bone in the center of each bone (Figure 9A and 9B). The longitudinal fractures are also associated with transverse fractures bisecting the anterior portion of the tibia at midshaft and slightly distal. As there are no signs of healing, but no differences in coloration, traditional fracture timing methodologies to distinguish peri- and postmortem were inconclusive. Moreover, there are pathological changes that have been observed in living diabetes patients including a visible loss of trabecular bone that can be observed in the individual's radiographs (Figure 9A). To assess if the acute fractures present in the lower limb bones were the result of fracture fragility or more simply, a postmortem artifact from natural drying processes80, a DXA scan of the left hip was obtained (Figure 10). The left hip is assessed since the longitudinal fractures were observed in the femora and tibiae and the lumbar spine was incomplete. The approach here was to ascertain if the BMD was sufficiently low that normal weight-bearing activities could cause the fractures observed. Total BMD was 1.299 g/cm2 with a corresponding t-score of 1.8 indicating bone insufficiency was not the cause of the longitudinal fractures. In addition, postmortem longitudinal cracking produces fracture lines that run along the grain of the bone and can produce fractures at perpendicular angles from one another84.
In Case Study 2, Figure 11 provides the results for a 13-year-old, female recovered from a clandestine grave with a suspected history of long-term abuse. Numerous antemortem fractures were evident and patterning was consistent with child abuse85. Current standards to assess malnutrition in juveniles include comparison of long bone lengths to a reference sample. The juvenile limb lengths for this individual were 355 mm and 300 mm for the left femur and tibia, respectively. These lengths are size-matched most closely with 9-year-old mean lengths (350 mm and 280 mm for femora and tibiae, respectively). This is consistent with a pronounced growth deficit for this individual86,87. Ruff's39 equation for femur and tibia lengths was used to estimate juvenile stature for the decedent. The estimated stature was 53.3 inches (136.2 cm) (95% CI: 51.1-55.5 inches). This was compared to the CDC 2000 growth curves for girls aged 2-2041. As seen in Figure 12, the decedent lies below the 3rd percentile for stature-for-age suggesting delayed growth well below most U.S. 13-year-old females. BMD was assessed to provide further insight into the degree of malnutrition as the association between BMD loss and poor nutrition is well established25,35,36. The lumbar spine was chosen for its completeness and larger composition of trabecular bone. The total BMD of the AP lumbar spine was measured at 0.660 g/cm2 with a z-score of -2.2 from the manufacturer’s database. The manufacturer’s database is an age and sex matched sample containing 1,948 individuals aged 3-20 years88. This z-score is consistent with low BMD for chronological age providing further evidence consistent with chronic malnutrition (Figure 13).
In Case Study 3, Figure 14 displays the BMD results of the lumbar spine for a 14-month-old infant with starvation suspected as the cause of death. The remains were still in early fresh stage of decomposition so articulation of epiphyses was not a concern and weight was 6.1 kg (13.4 lbs). For comparison purposes, the Gomez and colleagues and Waterlow classification systems were employed to estimate malnutrition from reference height and age measurements. Following the Gomez and colleagues89 equation:
Percent of reference weight for age = ((patient weight) / (weight of normal child of same age)) * 100
where the weight of normal child of same age is taken from a reference population. The infant in this case measured at 38% weight for age of the reference sample from Gomez and colleagues89, which is equivalent to Grade III (severe malnutrition). The Waterlow90 classification system places 38% as severe wasting, but without stunting as height was within the normal range. The total BMD was measured at 0.190 g/cm2 while the age-matched reference group has an average total BMD of the lumbar spine of 0.399 +/- 0.040 g/cm2 45. The z-score was calculated as:
z-score = ((Measured BMD – Age Matched Mean BMD) / Population SD)
and was -5.225 with the age-matched mean from a 1-year-old reference population of 40 infants. The reference data was produced from a longitudinal study by Braillon and coworkers91 that has been validated in the literature for DXA spine BMD measures49,92. Moreover, a study by Gallo and colleagues suggests the infant BMD observed is below the 3rd percentile of spine BMD for age for 12-month olds92. Any score below -2 is considered low BMD for chronological age placing the infant in the 0.1 percentile of the normal population (Figure 13). For comparison, the weight of the infant (6.1 kg) was plotted on the CDC 2000 growth curve chart for males aged 0-341. As seen in Figure 15, the infant falls well below the 3rd percentile for weight-for-age, which is consistent with the DXA z-score well below the -2 for the low end of normal individuals.

Figure 1: Orientation and placement of lumbar spine segments, L1-L4 for scanning: (A) shows proper orientation for scanning with spinous processes oriented downwards (corresponds to step 2.2.3); (B) correct location for scanning with laser line bisecting vertebrate bodies and no contact between vertebrate bodies and black dot represents the crosshairs (corresponds to step 2.2.4). Arrow indicates direction to head of scanner. Please click here to view a larger version of this figure.

Figure 2: Successful AP lumbar spine scan ideal for analysis. Corresponds to step 2.2.7.

Figure 3: Placement of hip joint (os coxa and femur) to recreate acetabulo-femur joint. (A) indicates the hip joint alignment for scanning with the femoral head in the acetabulum and femoral head and greater trochanter in the same plane parallel to the scanning table (step 2.3.3) and the black dot indicates the location of crosshairs for correct table placement (step 2.3.5). (B) illustrates the degree of medial rotation of the femur appropriate for scanning (step 2.3.4). Please click here to view a larger version of this figure.

Figure 4: Successful left hip scan ideal for analysis. Notice that the os coxa does not extend below the femoral neck. Ensure placement of the joint does not have the iliac tuberosity inferior to the femoral neck (step 2.3.8).

Figure 5: An example of a successful AP lumbar spine scan. L1 – L4 indicates proper placement of vertebral lines between each vertebra (step 3.1.1).
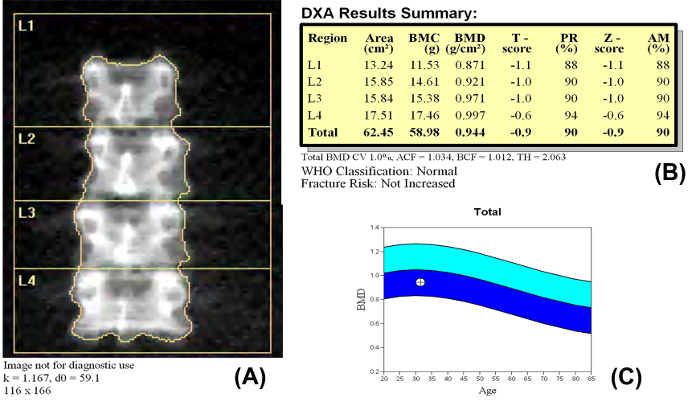
Figure 6: BMD results from an AP lumbar spine analysis (step 3.1.4). The results presented here are from a deceased white female, 31 years of age, and 64 inches tall. Report has been anonymized for publication. (A) presents image of properly scanned lumbar vertebrae separated by software placed vertebral lines; (B) scan results listing the individual vertebrae and total BMD scores as well as the t- and z-scores for the individual. The t- and z-scores were obtained using the WHO reference database for white females; (C) BMD vs. Age graph represents where the individual's BMD score (cross-hatch circle) falls within the range of average adult females in the WHO database.83 The darker blue shading represents the acceptable range above the mean and the lighter blue shading represents the acceptable range below the mean, or the two tails of the bell curve around the mean in a normal distribution curve. Please click here to view a larger version of this figure.

Figure 7: Screen displays an example of a successful hip scan with the femoral midline bisecting the femoral head to just inferior the trochanteric region. The femoral neck box should be at an angle to capture the full femoral neck angle (step 3.2.2).

Figure 8: BMD results from a left hip analysis (step 3.2.5). The results presented here are from a deceased white female, 31 years of age, 64 inches tall. Report has been anonymized for publication. (A) presents image of properly scanned left hip with midline accurately placed with no additional bone included from os coxa; (B) scan results listing the neck, trochanteric region (Troch), the intertrochanteric region (Inter), and total BMD scores as well as the t- and z-scores for the individual. The t- and z-scores were obtained using the WHO reference database for white females. This individual is classified as osteopenic with increased fracture risk using the WHO references83; (C) BMD vs. Age graph represents where the individual's BMD score (cross-hatch circle) falls within the acceptable range albeit on the low end of peak adult females in the WHO database. The darker blue shading represents the acceptable range above the mean and the lighter blue shading represents the acceptable range below the mean, or the two tails of the bell curve around the mean in a normal distribution curve. Please click here to view a larger version of this figure.

Figure 9: Radiographs for Case Study 1. (A) shows the longitudinal fractures of the right femur and (B) the transverse stress fracture of the right tibia. Also note the reduced radiopaque quality of the proximal femur. Please click here to view a larger version of this figure.

Figure 10: BMD results for Case Study 1. The results presented here are from a deceased white male, 40 years of age, approximately 72 inches tall. Report has been anonymized for publication. (A) presents image of left hip scan; (B) scan results presenting the neck, trochanteric region (Troch), the intertrochanteric region (Inter), and total BMD scores as well as the t- and z-scores for the Case Study 1. The t- and z-scores were obtained using the WHO reference database for white males.83 This individual is classified as normal using the WHO references; (C) BMD vs. Age graph represents where the individual's BMD score (cross-hatch circle) falls within the acceptable range of adult males in the WHO database. The darker blue shading represents the acceptable range above the mean and the lighter blue shading represents the acceptable range below the mean, or the two tails of the bell curve around the mean in a normal distribution curve. Please click here to view a larger version of this figure.

Figure 11: BMD results for Case Study 2. The results presented here are from a deceased white female, 13 years of age, approximately 53 inches tall. Report has been anonymized for publication. (A) presents scan of AP lumbar vertebrae for Case Study 2 separated by software placed vertebral lines; (B) scan results present the individual vertebrae and total BMD scores as well as the z-scores for the individual. Z-scores only are presented in juvenile cases because they were obtained using the WHO reference database for age- and sex-matched individuals; (C) BMD vs. Age graph represents where the individual's BMD score (cross-hatch circle) falls below the range (z-score=-2.2) of 13-year-old white females in the manufacturer's database.88 The darker blue shading represents the acceptable range above the mean and the lighter blue shading represents the acceptable range below the mean, or the two tails of the bell curve around the mean in a normal distribution curve. Please click here to view a larger version of this figure.

Figure 12: Growth chart illustrating the delayed maturation of the 13-year-old female decedent.41 The black dot represents the mean estimated stature and the black lines represent the 95% confidence interval for the stature equation. The individual lies below the 3rd percentile for stature-for-age within the entire range of the CI. Please click here to view a larger version of this figure.

Figure 13: Assignment of case study 3 infant z-score relative to the normal population distribution. All values below the red center box for the normal population measures are considered to indicate low BMD for chronological age. Please click here to view a larger version of this figure.

Figure 14: BMD results for Case Study 3. The results presented here are from a deceased male infant, 14 months of age. Report has been anonymized for publication. (A) presents scan of AP lumbar vertebrae for Case Study 3 separated bone map of vertebral body epiphyses and surrounding vertebral processes; (B) scan results present the individual vertebrae and total BMD scores. The manufacturer's database used by this software did not have any age- and sex-matched information for infants younger than three years of age. References from Braillon and colleagues91 were used to calculate the z-score.

Figure 15: Growth chart illustrating the severe wasting of the 14-month-old infant.41 The black dot represents the 6.1 kg (13.4 lbs) weight of the infant. The infant falls well below the 3rd percentile for weight-for-age. Please click here to view a larger version of this figure.
