

Summary
The chronic administration of isoproterenol via an implanted osmotic pump has been used widely to mimic advanced heart failure in mice. Here, we describe detailed methods in surgical mini-pump implantation for the continuous isoproterenol administration over 3 weeks, as well as, echocardiographic assessment for the successful model creation.
Abstract
Isoproterenol (ISO), is a non-selective beta-adrenergic agonist, that is used widely to induce cardiac injury in mice. While the acute model mimics stress-induced cardiomyopathy, the chronic model, administered through an osmotic pump, mimics advanced heart failure in humans. The purpose of the described protocol is to create the chronic ISO-induced heart failure model in mice using an implanted mini-pump. This protocol has been used to induce heart failure in 100+ strains of inbred mice. Techniques on surgical pump implantation are described in detail and may be relevant to anyone interested in creating a heart failure model in mice. In addition, the weekly cardiac remodeling changes based on echocardiographic parameters for each strain and expected time to model development are presented. In summary, the method is simple and reproducible. Continuous ISO administered via the implanted mini-pump over 3 to 4 weeks is sufficient to induce cardiac remodeling. Finally, the success for ISO model creation may be assessed in vivo by serial echocardiography demonstrating hypertrophy, ventricular dilation, and dysfunction.
Introduction
Heart failure with reduced ejection fraction (HFrEF) is accompanied by a well-recognized compensatory response of the sympathetic nervous system to maintain cardiovascular homeostasis1. Hemodynamic stress and deleterious effects on the heart and circulation were observed with chronic activation. These have become the cornerstone of contemporary pharmacotherapy for heart failure and are important mechanisms in the progression of heart failure and therapeutic antagonism of neurohormonal systems1.
Several mouse models are available for basic investigations of heart failure. Genetic models are attractive for exploring molecular therapies and investigating signaling pathways. However, these models may not be relevant to common forms of heart failure. Other common models include left anterior descending (LAD) artery ligation, transaortic constriction (TAC), and isoproterenol (ISO), each aiming at a different pathological etiology2,3,4,5,6. LAD artery ligation induces an anterior wall myocardial infarction thus creating a model specific for ischemic cardiomyopathy. TAC induces acute pressure overload to create a hypertensive model of heart failure. Although the pressure gradient can be measured, allowing for the stratification of hypertrophy, the acute onset of hypertension lacks direct clinical relevance4. Both LAD and TAC models require a high level of surgical expertise to execute. Acute ISO model of heart failure mimics stress-induced cardiomyopathy, also known as Takotsubo disease, which is characterized by a marked increase in catecholamines and activity in the left ventricle that mimics acute myocardial infarction7,8. In contrast, chronic ISO models of heart failure present symptoms characteristics of advanced heart failure, with chronically elevated levels of catecholamines1. The advantages of the chronic ISO model are that it provides chronic adrenergic stimulation that mimics advanced heart failure and that it is relatively easy to create. The investigator should choose a model that best recapitulates their pathology of interest.
The overall goal of this method is to induce heart failure in mice using an implanted mini pump that releases ISO continuously to mimic chronic sympathetic activation found in heart failure patients1. The method is simple and reproducible. Although there is clear variation among mouse strains, ISO administered over 3 to 4 weeks at 30 mg/kg/day is sufficient to induce cardiac remodeling in most mice. Specifically, ISO leads to a pro-hypertrophic compensatory phase during week 1 followed by wall thinning, ventricular dilation and decrease in systolic function by week 2 and 32. Success for the ISO model creation can be assessed in vivo by serial echocardiography demonstrating hypertrophy, dilation, and ventricular dysfunction, as well as ex vivo via histological and molecular assessment of harvested cardiac tissue for intramyocardial lipid accumulation, fibrosis, ER stress, apoptosis, and gene expression9,10,11,12.
Subscription Required. Please recommend JoVE to your librarian.
Protocol
This protocol adheres to the animal care guidelines of the University of California, Los Angeles (ARC protocol #2010-075). Readers are advised to adhere to their own IACUC-approved protocol, as peri-procedure mouse care and analgesia management may be institution-specific.
1. Preparation of isoproterenol osmotic pump
NOTE: This procedure has been applied successfully on 9+ week-old female mice weighing 18+ g from over 100 inbred mouse strains, as well as, in male mice in a subset of strains. There is no maximum body weight limit for this procedure. Always include age-matched controls, as it is unknown whether the age of treatment affects isoproterenol-induced susceptibility to heart failure development.
- Weigh and record the body weight for each mouse.
- Calculate the appropriate amount and concentration of isoproterenol for each mouse (See Table 1 ; Supplemental File).
NOTE: The osmotic pumps used in this experiment (Table of Materials) have a reservoir volume of 100 µL and are designed to deliver drugs at continuous flow rates for up to 28 days. Prepare an extra 20 µL of isoproterenol solution per pump to account for the volume loss in the filling tube during pump loading. - Weigh out the appropriate amount of isoproterenol (Table 1) using an analytical balance and dissolve it in 120 µL of sterile 0.9% NaCl solution. Pipette vigorously or vortex for 1 min to completely solubilize isoproterenol.
NOTE: Prepare the osmotic pumps in a laboratory biosafety cabinet. Pumps should be handled with surgical gloves. Sterile technique is recommended throughout the preparation of the osmotic pumps and during the surgical implantation procedure. - Weigh and record the empty osmotic pump together with its flow moderator and then remove the flow moderator.
- Aspirate 120 µL of isoproterenol solution into a 1.0 mL syringe and attach the 27-gauge blunt-tipped filling tube provided with the osmotic pumps.
NOTE: Make sure the syringe and filling tube are free of air bubbles. - While holding the pump in the upright position, insert the filling tube through the pump opening at the top until the tip of the filling tube sits near the bottom of the pump reservoir.
- Load the osmotic pump by pushing the syringe plunger slowly until the isoproterenol solution fills up to the pump opening.
- Carefully remove the filling tube and wipe off the excess solution.
- Insert back the flow moderator to close the pump and wipe off any excess solution.
- Confirm that over 90% of the reservoir volume has been filled by reweighing the osmotic pump.
NOTE: Control pumps are prepared in the same manner by filling the pump reservoir with sterile 0.9% NaCl solution.
2. Preparation of surgical instruments
- Clean all surgical instruments, including fiber optic O-ring light microscope illuminator, 2 forceps, needle holder, hot bead sterilizers, glass beads, and scissors (Table of Materials).
- Autoclave surgical instruments at 121° C for 30 min to sterilize instruments prior to surgery.
3. Isoproterenol osmotic pump surgical implantation
- Induce anesthesia by placing the mouse in an induction chamber with 3% isoflurane in 95% O2 and 5% CO2. Maintain anesthesia with 2% isoflurane via a nosecone.
- Administer 5 mg/kg carprofen s.c. to the scruff of the neck between the shoulder blades for analgesia.
- Place ophthalmic ointment on the eyes to prevent corneal dehydration.
- Check the depth of anesthesia by monitoring the respiration rate, toe pinch reflex, and color of the mucous membrane.
- Place the mouse in a supine position on a heated pad. Remove hair from the lower abdomen and disinfect the skin with betadine or chlorhexidine.
NOTE: To minimize post-operative infection, ensure that the surgical field is free of incident hair. - Use a pair of surgical scissors to cut a 1 cm-long midline skin incision. Use a pair of blunt-ended scissors to carefully dissect the skin from the underlying peritoneal walls.
NOTE: An intraperitoneal delivery is preferred to accommodate the size of the pump. - Pull the peritoneal walls away from the underlying bowel with forceps and cut a 0.8 cm hole in the peritoneal walls using fine surgical scissors.
- Insert the osmotic pump into the peritoneal cavity with the flow moderator end first.
- Close the hold in the peritoneal walls using 5.0 absorbable sutures in an interrupted fashion. Use 6.0 non-absorbable sutures to close the skin incision in an interrupted fashion.
- Place the mouse in a dedicated incubator to keep it warm and dry during recovery. Assess recovery from anesthesia by monitoring the mouse every 30 mins in the first two hours for return of normal breathing and movement.
- Once the mouse has fully recovered from anesthesia, return it to routine housing. Continue to monitor the animal for complications daily up to 3 days and then every 2 to 3 days thereafter until the end of the experiment.
NOTE: Animals should be monitored for evidence of post-operative pain or infection, signs of weight loss, lack of mobility, abnormal posture, failure to groom, and excessive licking or biting of the incision area. - Administer carprofen 5mg/kg s.c. every 24 h for up to 48 h and thereafter as needed.
- Administer 0.25 mg/mL amoxicillin in drinking water for 5 days to prevent surgical site infections.
- Remove non-absorbable sutures after 7 to 10 days.
4. Echocardiographic assessment under anesthesia
NOTE: Echocardiographic assessment can be performed repeatedly to monitor serial cardiac remodeling over several weeks. We performed echocardiographic measurements at weekly intervals over 3 weeks.
- Induce anesthesia in an induction chamber at 1.25% to 1.5% of isoflurane. Once appropriately sedated, secure the mouse onto the echocardiography platform with tape allowing the mouse to continue receiving anesthesia through a nose cone.
- Decrease isoflurane to a maintenance dosage of 1% to minimize negative chronotropic and inotropic effects of over-sedation. Take note of respiratory and heart rates throughout the study and adjust isoflurane dosage as needed.
- Remove the chest hair with a depilatory lotion and wipe the chest free of hair.
- Place the ultrasound gel on the chest and position the ultrasound probe to image the heart.
- In B-mode, image the left ventricle (LV) in the parasternal long-axis view. Adjust the echocardiography platform to align the aortic valve and the LV apex in the plane of the ultrasound beam.
- Tilt the echocardiography platform to place the LV long axis at 90 degrees to the ultrasound beam and the LV maximum diameter at the center of the image.
- Image the LV short axis by turning the ultrasound probe 90 degrees.
- In M-mode measure LV wall thickness and internal dimensions.
- Place the mouse back into the cage. Monitor for return of normal breathing and spontaneous body movements.
Subscription Required. Please recommend JoVE to your librarian.
Representative Results
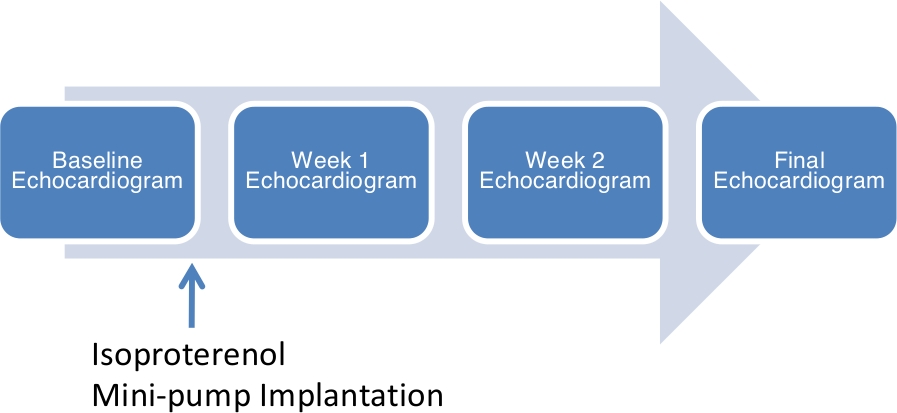
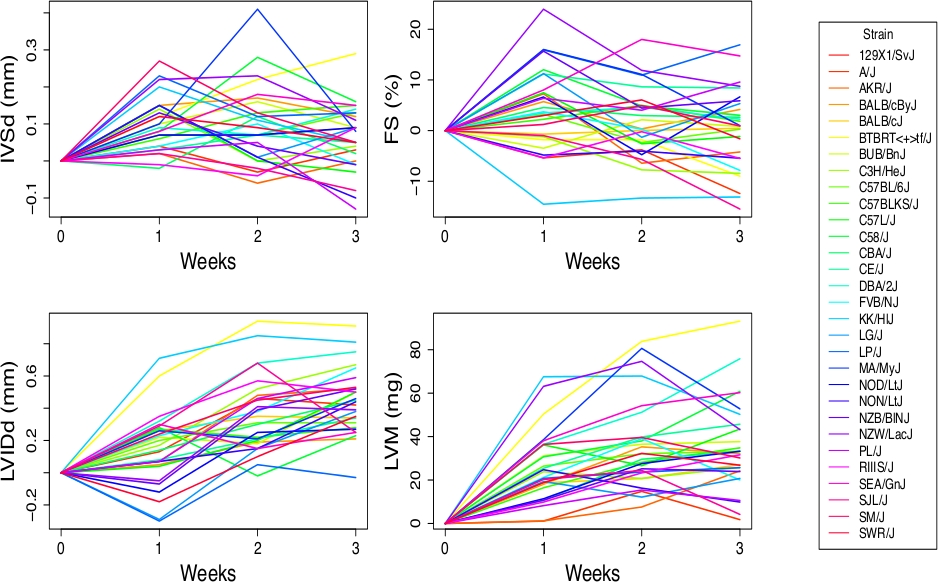
In our previously published study, we administered an ISO dosage of 30 mg/kg/d over 21 days via the osmotic pump across 105 Hybrid Mouse Diversity Panel (HMDP) strains2,13. We assessed outcomes using echocardiogram performed at baseline, week 1, 2 and 3 of ISO treatment (Figure 1). Similar to a prior study where the authors studied the impact of isoproterenol among 23 mouse strains14, we observed striking inter-strain variation among echocardiographic parameters. The summary of weekly changes based on echocardiographic parameters and expected time to model development is presented (Figure 2 and Figure 3)2,15. Although variations were observed among mouse strains, on average, interventricular septal wall thickness at end diastole (IVSd) and fractional shortening (FS) increase in the first week but decrease by later time points; left ventricular internal diameter at end diastole (LVIDd) and left ventricular mass (LVM) increase over a period of 3 weeks (Figure 3). These findings are consistent with a pro-hypertrophic compensatory phase during week 1 of isoproterenol followed by wall thinning, ventricular dilation and decrease in systolic function. Our previously published study also demonstrated the upregulation of several gene subsets associated with left ventricular hypertrophy, including fibrotic marker Lgals3 and heart failure marker Nppb by week 32. Other differentially regulated genes include those involved in angiogenesis, secreted signal glycoprotein, polysaccharide binding, actin cytoskeleton, chemokine signaling pathway, proteinaceous extracellular matrix, and collagen2. These results are corroborated by echocardiographic and histological findings: mouse hearts demonstrated visibly larger left ventricular chamber dimensions under ISO and greater amounts of fibrosis under ISO treatment relative to saline control (Figure 4).

Figure 1: Chronic Isoproterenol (ISO)-Induced Heart Failure Model via Mini-Pump.
This figure has been adapted with permission from Wang et al.2 and Chang et al.15 Please click here to view a larger version of this figure.

Figure 2: Variation in echocardiographic measures of cardiac structure and function among the Hybrid Mouse Diversity Panel (HMDP) mouse strains.
Black bars represent measurements under the baseline condition in ranked order. White bars represent measurements after 3 weeks of continuous ISO infusion. IVSd = interventricular septal wall thickness; LVIDd = left ventricular internal diameter at end diastole; LVM = left ventricular mass; FS = fractional shortening. Error bars represent the standard errors of the means (SEM). This figure has been adapted with permission from Wang et al.2 and Chang et al.15.

Figure 3: The average changes in echocardiographic measures compared to baseline at each ISO time point for each classical inbred strain.
This figure has been adapted with permission from Wang et al.2 and Chang et al.15. Please click here to view a larger version of this figure.

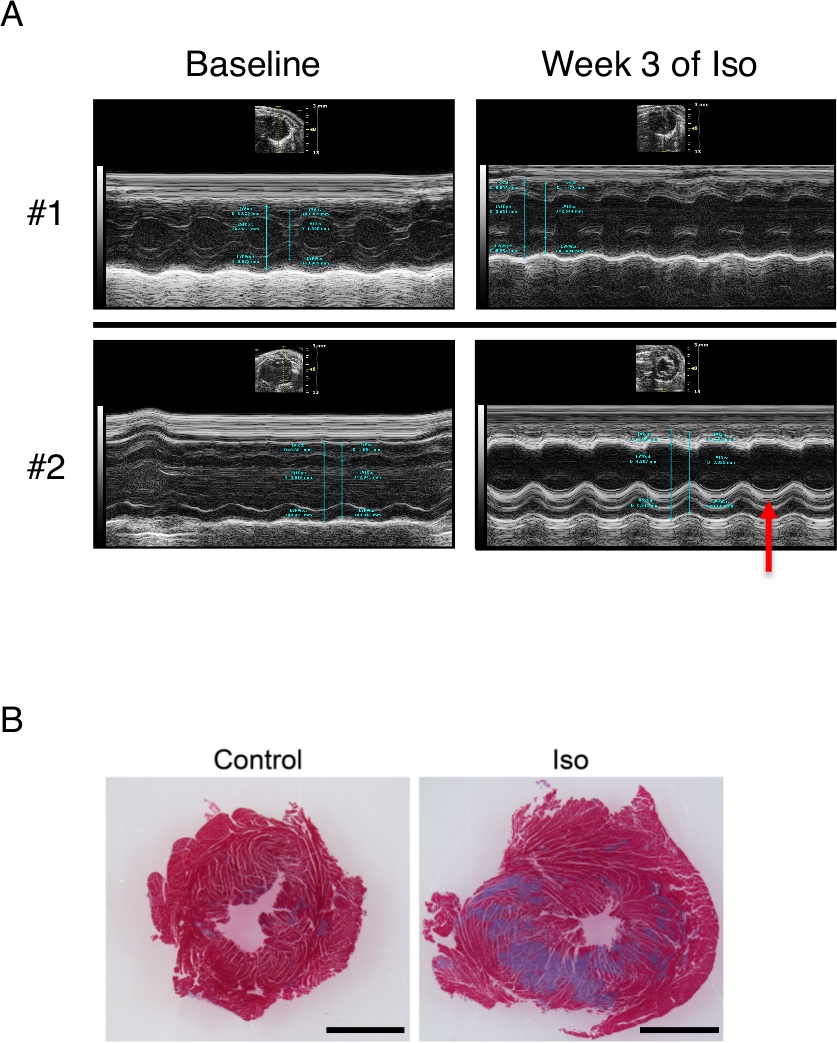
Figure 4: Echocardiographic and histologic changes after chronic isoproterenol infusion.
(A) Representative M-mode echocardiogram images from 2 mice at baseline and at week 3 of isoproterenol are shown. Note enlargement of the left ventricular internal dimensions in both mice as well as the development of endocardial fibrosis (red arrow) in mouse #2. (B) Masson's trichrome stain of the left ventricle in the short axis demonstrates extensive fibrosis with isoproterenol treatment (scale bar: 2 mm). Please click here to view a larger version of this figure.
| Body Weight (g) | Daily dosage (μg/day) | Flow Rate (μL/day) | Concentration (μL/day) | Isoproterenol (mg/120 µl) |
| 20 | 600 | 2.64 | 227 | 27.3 |
| 21 | 630 | 2.64 | 239 | 28.6 |
| 22 | 660 | 2.64 | 250 | 30 |
| 23 | 690 | 2.64 | 261 | 31.4 |
| 24 | 720 | 2.64 | 273 | 32.7 |
| 25 | 750 | 2.64 | 284 | 34.1 |
| 26 | 780 | 2.64 | 295 | 35.4 |
| 27 | 810 | 2.64 | 307 | 36.8 |
| 28 | 840 | 2.64 | 318 | 38.2 |
| 29 | 870 | 2.64 | 330 | 39.5 |
| 30 | 900 | 2.64 | 341 | 40.9 |
Table 1: Isoproterenol concentration and preparation for representative body weights at the osmotic pump rate of 30 mg/kg/d. This table has been adapted with permission from Wang et al.2 and Chang et al.15.
Supplemental File. Please click here to download this file.
Subscription Required. Please recommend JoVE to your librarian.
Discussion
We have applied this method to over 100+ strains of inbred mice to assess cardiac outcomes due to chronic beta-adrenergic stimulation2,13. Significant differences in susceptibility to isoproterenol are known to exist among mouse strains and may be customized to the strain of interest as needed16. This may be due to the variation in beta-adrenergic receptor function between mouse strains17, strain-dependent differences in autonomic nervous system activity16, beta-adrenergic receptor (beta-AR) density and/or coupling17 and other genetic differences among strains. Based on in vivo serial echocardiography as well as ex vivo cardiac tissue histology and gene expression with and without ISO, chronic isoproterenol treatment induced striking differences spanning from cellular processes, extracellular matrix to inflammatory responses2,13. The following considerations may be relevant to the application of this heart failure model.
Close to 30% of mice implanted with isoproterenol osmotic pump died before the end of the experimental protocol2,13. Of these, over 90% died within the first 48 hours after pump implantation. The deaths appeared strain specific, with BXA-12/PgnJ, BXD-34/TyJ, BTBRT<+>tf/J, NZW/LacJ, BXD40/TyJ, and BALB/cJ being the most susceptible strains. Moreover, we observed that mice weighing < 20 g had a higher early post-operative mortality (death within 48 h). Allowing mice to mature to at least 9 to 10 weeks of age or > 20 g may minimize early post-operative mortality. Therefore, it may be important to account for strain-specific differences and early post-operative mortality when planning an experiment. We did not perform an autopsy to determine the cause of death. Hence, we are not able to determine the failure rate of the osmotic pumps. Of the mice that were sacrificed we detected no visual defects.
Isoflurane is known to be negatively chronotropic and inotropic. Care should be taken to minimize sedation and impact of isoflurane on echocardiographic measurements. If the sternum casts a bony shadow and degrades image qualities, reposition the mouse to image the heart through a different intercostal space. If the interventricular wall thickness measurement is complicated by the presence of the right ventricular wall, reimage through a different intercostal space to minimize poorly delineated borders. Accurate measurements are critical to downstream comparative analyses.
There exists literature documenting the use of osmotic minipumps in rats18,19. Readers should note that this protocol has only been used with mice and that other literature should be referenced for experimentation with other species.
Past literature suggests that daily injections of isoproterenol and continuous administration via osmotic pumps cause similar ventricular weight relative to body weight20. However, there are differences in hemodynamics. Daily injections cause immediate hypotension and tachycardia followed by rebound hypertension within a few hours. Continuous administration causes immediate hypotension on the day of pump implantation followed by normalization of blood pressure to mild hypertension by day 220. The overall hemodynamic trends more closely mimic chronically activated sympathetic hormones in heart failure patients.
At week 1 of isoproterenol, contractility was increased or supernormal. By week 2 and 3, contractility was back to normal for most strains and decreased for some strains. In the background of ongoing isoproterenol, normal contractility as measured by fractional shortening (FS) and ejection fraction (EF) may, in fact, represent impaired contractile reserve. If the investigator desires to induce a more profound degree of cardiac impairment, one may increase the ISO dosage or lengthen the ISO treatment period to 4 weeks, while weighing the risk of increased post-operative mortality. Finally, the data we presented were based on female mice only. Female mice have demonstrated higher post-ischemic contractile function and lesser ATP-depletion in an ischemia reperfusion injury model as compared to male mice21. Moreover, in a chronic ISO model, male mice have demonstrated an elevated heart to body weight ratio and reduced total norepinephrine levels in parotid and submaxillary glands as compared to females22. The user may need to consider gender-based differences in the observed outcomes when applying this approach to females and males.
Subscription Required. Please recommend JoVE to your librarian.
Disclosures
The authors have nothing to disclose.
Acknowledgments
The authors acknowledge NIH K08 HL133491 for funding support.
Materials
| Name | Company | Catalog Number | Comments |
| Micro-Osmotic Pump System with Flow Moderator in Place | Alzet | Model 1004 | Includes filling tube, flow moderator and pump body |
| (-)-Isoproterenol hydrochloride | Sigma-Aldrich | 16504-1G | (-)-Isoproterenol hydrochloride is a powder that needs to be stored at -20°C. |
| 1 ml sterile syringe | VWR | BD309602 | |
| 30 W LED Fiber optic O-ring light microscope illuminator | AmScope | SKU: LED-30WR | |
| 5-0 COATED VICRYL (polyglactin 910) Suture | Ethicon | J303H | 5-0, absorbable |
| Fine Scissors - Sharp | FST | 14060-09 | |
| Glass beads | FST | 18000-46 | |
| Hot bead sterilizers | FST | 18000-50 | |
| Iris forceps | WPI | 15915 | |
| Look Sharpoint 6-0, 18" Black Nylon Monofilament Suture | LOOK | AA-2176 | 6-0, non-absorbable |
| Needle holder | WPI | 15926 | |
| Normal Saline, 0.9% NaCl | Fisher | 89167-772 |
References
- Hartupee, J., Mann, D. L. Neurohormonal activation in heart failure with reduced ejection fraction. Nature Review Cardiology. 14 (1), 30-38 (2017).
- Wang, J. J., et al. Genetic Dissection of Cardiac Remodeling in an Isoproterenol-Induced Heart Failure Mouse Model. PLoS Genetics. 12 (7), 1006038 (2016).
- Balakumar, P., Singh, A. P., Singh, M.
- Patten, R. D., Hall-Porter, M. R. Small animal models of heart failure: development of novel therapies, past and present. Circulation: Heart Failure. 2 (2), 138-144 (2009).
- Huang, W. Y., Aramburu, J., Douglas, P. S., Izumo, S. Transgenic expression of green fluorescence protein can cause dilated cardiomyopathy. Nature Medicine. 6 (5), 482-483 (2000).
- Breckenridge, R. Heart failure and mouse models. Disease Model and Mechanism. 3 (3-4), 138-143 (2010).
- Wittstein, I. S., et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. New England Journal of Medicine. 352 (6), 539-548 (2005).
- Templin, C., et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. New England Journal of Medicine. 373 (10), 929-938 (2015).
- Shao, Y., et al. A mouse model reveals an important role for catecholamine-induced lipotoxicity in the pathogenesis of stress-induced cardiomyopathy. European Journal of Heart Failure. 15 (1), 9-22 (2013).
- Kudej, R. K., et al. Effects of chronic beta-adrenergic receptor stimulation in mice. Journal of Molecular Cell Cardiology. 29 (10), 2735-2746 (1997).
- Zhuo, X. Z., et al. Isoproterenol instigates cardiomyocyte apoptosis and heart failure via AMPK inactivation-mediated endoplasmic reticulum stress. Apoptosis. 18 (7), 800-810 (2013).
- El-Demerdash, E., Awad, A. S., Taha, R. M., El-Hady, A. M., Sayed-Ahmed, M. M. Probucol attenuates oxidative stress and energy decline in isoproterenol-induced heart failure in rat. Pharmacology Research. 51 (4), 311-318 (2005).
- Rau, C. D., et al. Mapping genetic contributions to cardiac pathology induced by Beta-adrenergic stimulation in mice. Circulation Cardiovascular Genetics. 8 (1), 40-49 (2015).
- Berthonneche, C., et al. Cardiovascular response to beta-adrenergic blockade or activation in 23 inbred mouse strains. PLoS One. 4 (8), 6610 (2009).
- Chang, S. C., Ren, S., Rau, C. D., Wang, J. J. Isoproterenol-Induced Heart Failure Mouse Model Using Osmotic Pump Implantation. Methods Molecular Biology. 1816, 207-220 (2018).
- Shusterman, V., et al. Strain-specific patterns of autonomic nervous system activity and heart failure susceptibility in mice. American Journal of Physiology-Heart Circulation Physiology. 282 (6), 2076-2083 (2002).
- Faulx, M. D., et al. Strain-dependent beta-adrenergic receptor function influences myocardial responses to isoproterenol stimulation in mice. American Journal of Physiology-Heart Circulation Physiology. 289 (1), 30-36 (2005).
- Zhang, G. X., et al. Cardiac oxidative stress in acute and chronic isoproterenol-infused rats. Cardiovascular Research. 65 (1), 230-238 (2005).
- Boluyt, M. O., et al. Isoproterenol infusion induces alterations in expression of hypertrophy-associated genes in rat heart. American Journal of Physiology. 269 (2), Pt 2 638-647 (1995).
- Hohimer, A. R., Davis, L. E., Hatton, D. C. Repeated daily injections and osmotic pump infusion of isoproterenol cause similar increases in cardiac mass but have different effects on blood pressure. Canadian Journal of Physiology and Pharmacology. 83 (2), 191-197 (2005).
- Cross, H. R., Murphy, E., Koch, W. J., Steenbergen, C. Male and female mice overexpressing the beta(2)-adrenergic receptor exhibit differences in ischemia/reperfusion injury: role of nitric oxide. Cardiovascular Research. 53 (2), 662-671 (2002).
- Klingman, G. I., McKay, G., Ward, A., Morse, L. Chronic isoproterenol treatment of mice: effects on catecholamines and rectal temperature. Journal of Pharmaceutical Sciences. 62 (5), 798-801 (1973).

{kind=link}
{kind=link}
{kind=link}