The presented protocol is an ongoing investigation. Table 1 depicts the protocol’s testing administration schedule. Representative results are presented to demonstrate the feasibility of collecting baseline/pre-injury and post-concussion data across a variety of performance domains known to be impacted by concussion in youth. A single case of a concussed youth who has completed all stages of the protocol is presented to demonstrate recovery trajectories across selected outcome measures. Figure 1 provides representative data of baseline/pre-injury to post-concussion cognitive performance, balance and post-concussion symptoms. Further, Figure 2, Figure 3 and Figure 4 demonstrate resting state HRV data along with pilot results indicating preliminary support to use resting state HRV as an indicator of recovery following concussion.

Table 1. Protocol testing administration schedule.
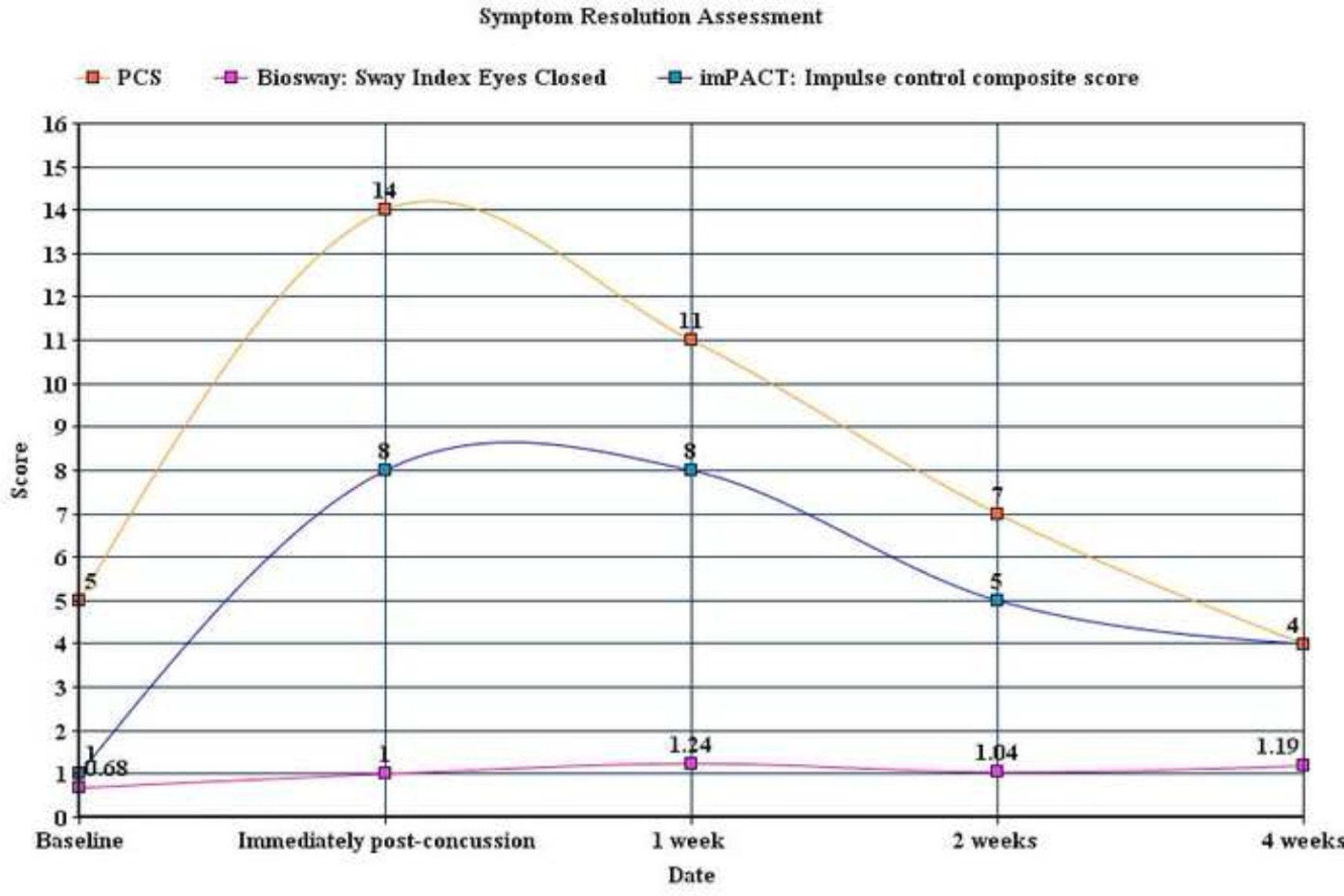
Figure 1. Baseline/pre-injury to post-concussion cognitive performance, balance and post-concussion symptoms. This single case indicates a decrease in cognitive and balance performance (larger score indicates decreased performance) immediately following concussion and an increase in post-concussion symptoms. Although post-concussion symptoms return to baseline levels at 4 weeks post-concussion, cognitive performance and balance deficits remain elevated (although cognitive performance is trending towards baseline levels). Note: Cognitive performance is presented as an impulse control composite score; balance is presented as sway index (standard deviation of sway angle according to center of gravity; the higher the sway index, the more unsteady the subject) during standing with eyes closed; and post-concussion symptoms (PCS) is presented as cumulative value of symptom severity ratings (using a 7-point likert scale; higher value indicates more severe symptoms). Please click here to view a larger version of this figure.
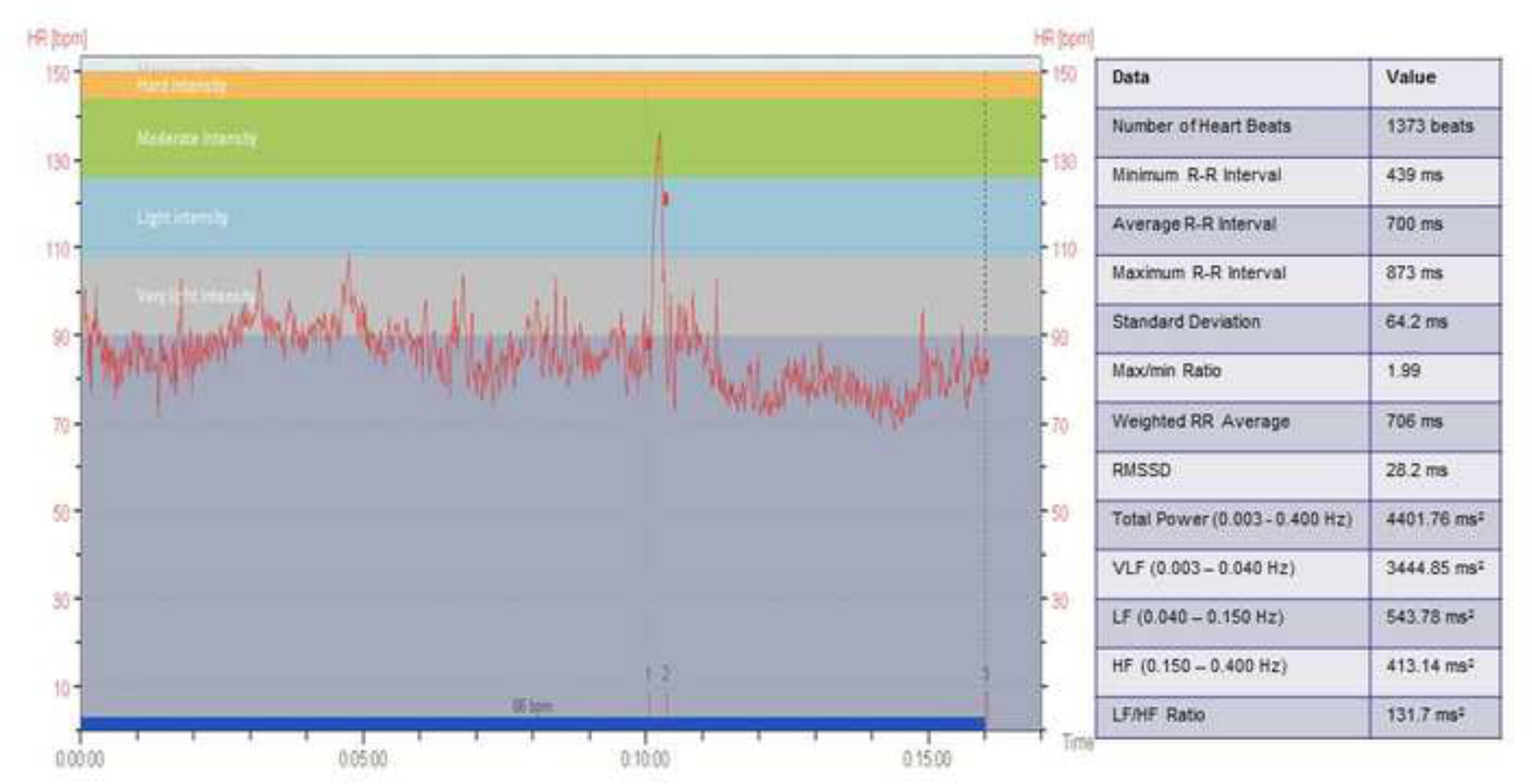
Figure 2. Example resting state heart rate variability (HRV) data. Heart rate (bpm) is shown across time for the entire 15 min HRV trial. Label 1 on the x-axis shows when the subject gets up from laying supine for 10 min. Label 2 shows when the subject begins sitting for the final 5 min of the trial. Label 3 shows when the entire trial is completed. Heart rate intensity is also shown with the corresponding colors. These data are then analyzed with Kubios software to give valuable information regarding HRV. The outcome measures analyzed Total Power (total spectrum power over frequencies between DC and 0.40 Hz), VLF (spectral power of the R-R intervals in the Very Low-Frequency range), LF (spectral power in the Low-Frequency range), HF (spectral power in the High-Frequency range which usually includes the respiratory frequency) are presented. Please click here to view a larger version of this figure.
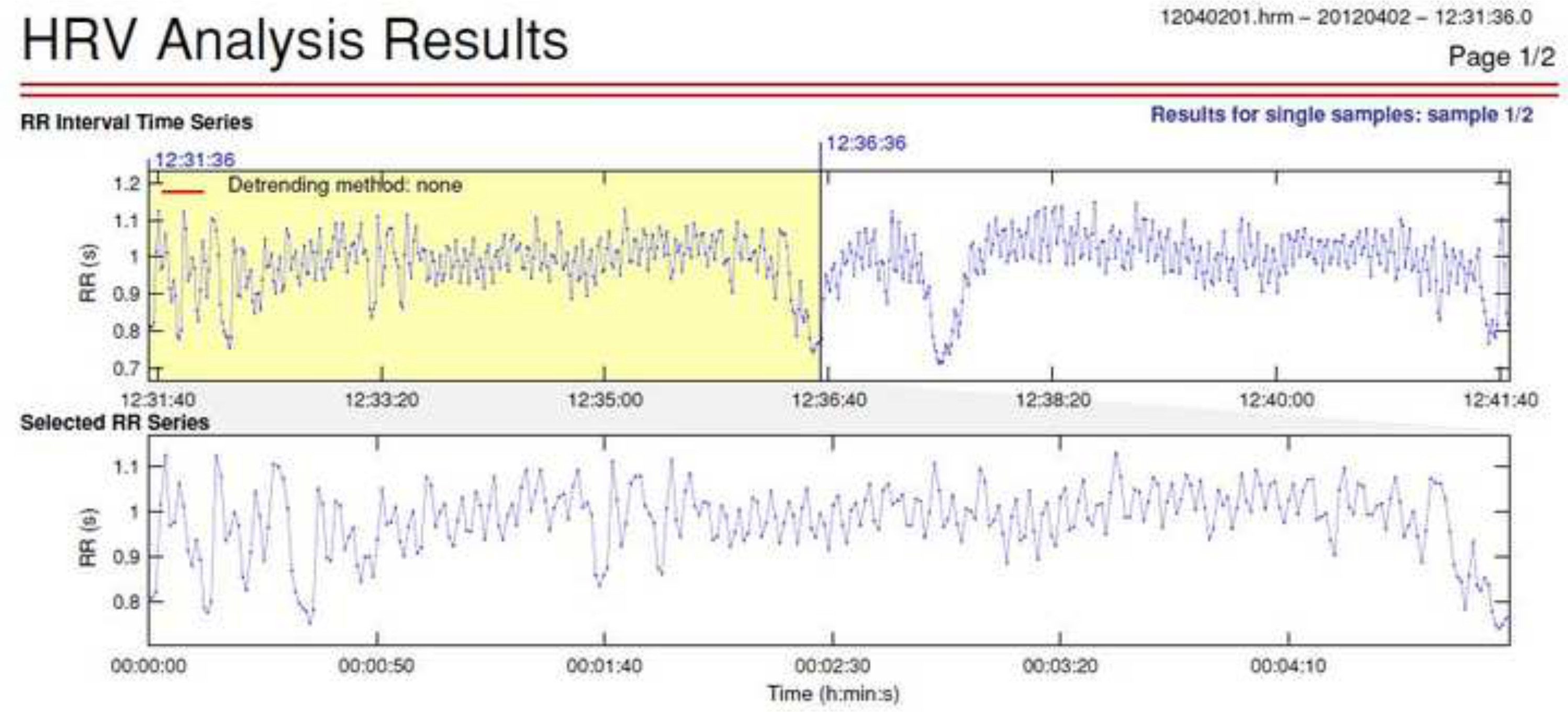
Figure 3. Example resting state HRV data. Total power heart rate variability reflects the total variance in heart rate pattern. Sympathetic activity is the primary contributor to total power frequency domain measures. A pilot study was conducted to obtain baseline and post-concussion measures of HRV frequency domain measures. 5 min selections of HRV were obtained from a longer sample and a low level artifact correction was applied. Please click here to view a larger version of this figure.

Figure 4. Example frequency domain measures of power for resting state HRV data. Frequency domain measures of power (msec2), using the Fast Fourier Transformation (FFT), were obtained at baseline and each re-test post-concussion. This figure indicates a total power of 3094 msec2.
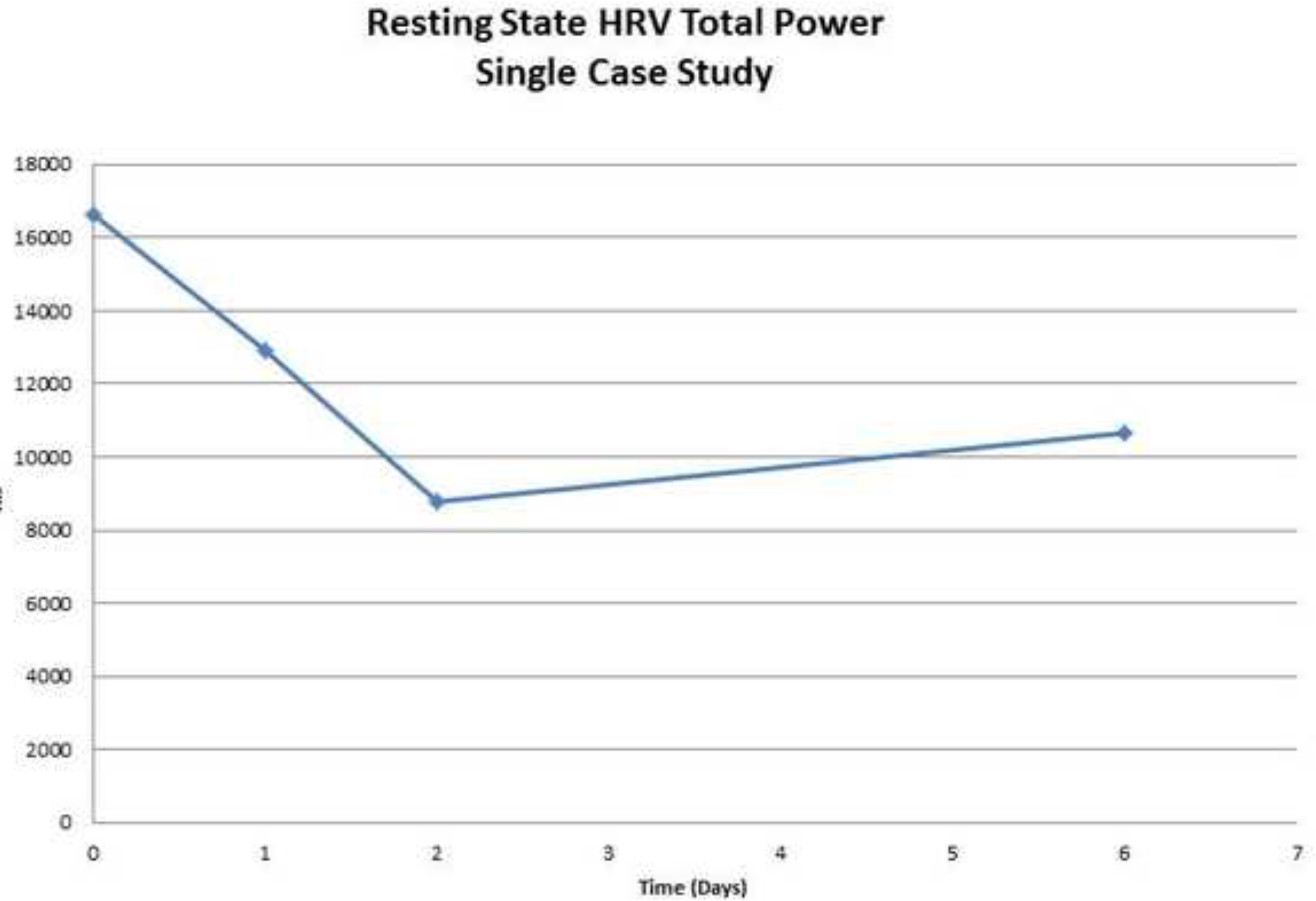
Figure 5. Example total power data across a single pilot participant before (day 0) and after a concussion (days 1-6). Total power (HRV) was graphed versus time. The participants demonstrated reduced total power (HRV) on day 1, day 2 and day 6 post-concussion. This pilot data demonstrates that the protocol for HRV collection, both at baseline and post-concussion, represents a feasible option for clinical examination. Data from this pilot study indicates that total power (HRV) is a tool that warrants further examination as a concussion assessment and management tool. Please click here to view a larger version of this figure.
