The animal operation was performed on each piglet, and the anatomic structures were identified, as shown in Figure 1 and Figure 2. Several structures were neatly dissected (SCM muscles and strap muscles) and carefully prepared (RLNs and VNs) according to the standardized procedure shown in Figure 1 and Figure 2. The tested SEDs in this study are shown in supplemental tables. Applying the standard procedures described in the Protocol section, the safety parameters of SEDs can be established in animal experiments.
Electrophysiological (EP) study
CIONM consists of three major parts: the stimulating electrode, the recording electrode, and the monitoring system (Figure 3A). After the CIONM system is ensured to be available, the signal change during the EP study can be well documented. (Figure 3D).
EP activation study: The EP activation study protocols are shown in Figure 4A. The safe activation distance is defined as single activation of the SED at a position greater than this distance without causing substantial EMG amplitude change. The APS EMG signal recordings of EP activation study are shown in Figure 4C. An example of demonstrating experimental results of EP activation study is shown in Table 1. The final interpretations are shown in Table 5.
EP cooling study: The EP cooling study protocols are shown in Figure 5A. The safe cooling time is defined as cooling for more than this time after a single activation of the SED that will not cause substantial EMG amplitude change. MTM of 1 s was performed immediately after a single activation of the SED, which determined whether the SED was safe or unsafe according to the occurrence of substantial EMG amplitude change. The APS EMG signal recordings of EP activation study are shown in Figure 5D. An example of demonstrating the experimental results of EP cooling study is shown in Table 2. The final interpretations are shown in Table 5.
Thermographic (TG) study
The standardized thermal imaging system setting is shown in Figure 6A. The temperature displays, the highest temperature mark ("+" sign), and the color scale are illustrated in Figure 6B. The background temperature of the experimental area is recorded as shown in Figure 6C. Strap muscles were prepared at a standard 5 mm thickness, which is shown in Figure 6D. The definition of the whole blade and one-third blade was demonstrated in Figure 6E,F.
TG activation study: The maximum temperature was tested with the whole blade in a dry environment; the results are shown in Table 3. The TG activation study contains four combinations: whole blade tests in a dry environment (Figure 7A,B), one-third blade tests in a dry environment (Figure 7C,D), whole blade tests in a wet environment (Figure 7E,F), and one-third blade tests in a wet environment (Figure 7G,H). Compared to the dry environment, heat splashing and lateral thermal spread tend to occur on the TG imaging screen in the wet environment. Different SEDs have different lateral thermal spread and smoke/splashing formation patterns when activated with a whole blade or one-third of a blade, according to their different hemostasis mechanisms. The thermal spread distance is defined as the farthest distance between the 60 °C isothermal line and the SED blade after a single activation. The experimental results are shown in Table 3. The final interpretations are shown in Table 5.
TG cooling study: The safe cooling time is defined as cooling for more than this time after a single activation of the SED, and it is completely lower than 60 °C on the TG screen. The MTM (Figure 8A) is a good cooling method in which the temperature is decreased rapidly under the TG imaging screen. MTM of 1 s was performed immediately after a single activation of the SED, and the temperature on the blade exceeding 60 °C or not determines whether the SED is safe or unsafe, respectively (Figure 8B). The experimental results, including minimum cooling time without MTM, blade temperature after MTM, and minimum cooling time with MTM, are shown in Table 4. The final interpretations are shown in Table 5.
Data interpretations
According to the data obtained in the experiments, the safety parameters of SED will be integrated into a table (Table 5 shows the data collected using Advanced bipolar SEDs (referenced as Device A) in the Table of Materials). Device A is one of the devices that is used for examination in this study. This data suggests that when surgeons use this SED, they should keep a sufficient safety distance and sufficient cooling time, adjust according to different operating environments and different grasping length, observe whether irregular thermal spread pattern occurs (smoke and splashing), and evaluate the temperature of the SED after a single activation and immediately after MTM is performed.
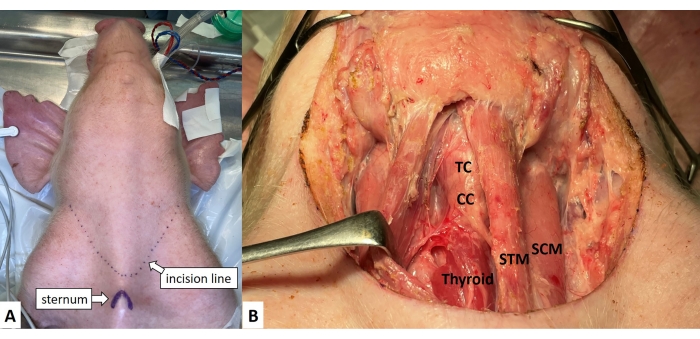
Figure 1: Skin Incision and dissection of the sternocleidomastoid muscles. (A) A 15 cm transverse cervical skin incision line is made 1 cm above the sternum. (B) The strap muscles are retracted laterally to visualize the thyroid cartilage, cricoid cartilage, tracheal rings, and thyroid gland. Abbreviations: SCM = sternocleidomastoid muscle, STM = strap muscles, TC = thyroid cartilage, CC = cricoid cartilage, Thyroid = thyroid gland. Please click here to view a larger version of this figure.
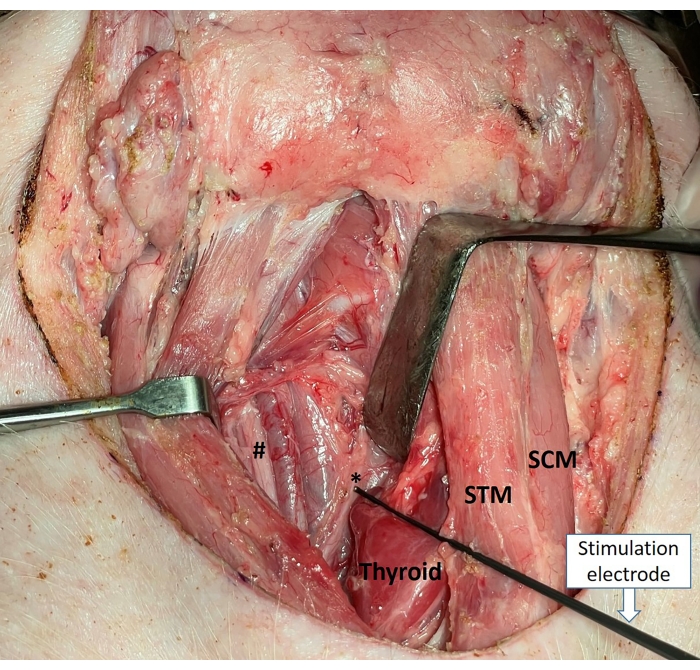
Figure 2: Identify and expose the RLNs (*) and VNs (#). Abbreviations: SCM = sternocleidomastoid muscle, S = strap muscles, TG = thyroid gland, RLN = recurrent laryngeal nerve, VN = vagus nerves. Please click here to view a larger version of this figure.
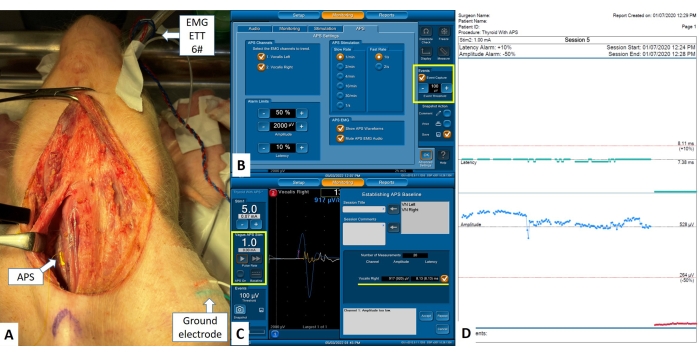
Figure 3: C-IONM settings and recordings. (A) Set up electrodes of C-IONM: recording electrodes- EMG endotracheal tube 6# was intubated; stimulating electrodes was installed on the VN (*); ground electrodes-electrodes were installed outside the surgical incision wound. All the electrodes were connected to the monitoring system. (B) The advanced settings of APS stimuli. (C) Set the current of stimulation and start to obtain the baseline in the Vagus APS Stim column, and the baseline latency and amplitude are tested and calculated automatically in the new window (establishing APS baseline). (D) The sample C-IONM report. Abbreviations: APS = automatic periodic stimulation, EMG = electromyography, ETT = endotracheal tube, C-IONM = continuous intraoperative neural monitoring, RLN = recurrent laryngeal nerve, VN = vagus nerves. Please click here to view a larger version of this figure.
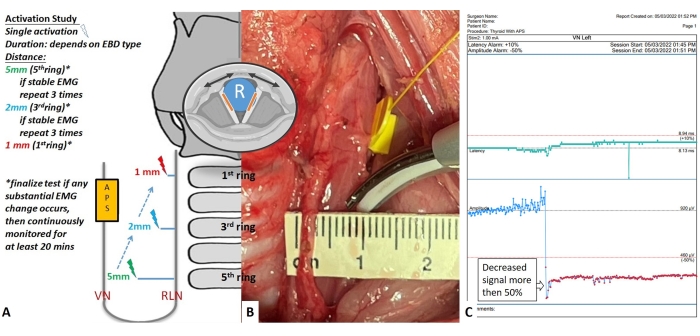
Figure 4: Flowchart of EP activation study protocols. (A) Single activation tests are performed on the RLN from the proximal (caudal) segments to the distal (cranial) segments at different distances. If the EMG response remained unchanged after the three activation tests at the 5 mm distance on the proximal segment, another test was performed at the 2 mm distance. If the EMG response remained stable after repeated tests at the 2 mm distance, final safety tests are performed at the 1 mm distance or by touching the SED tip with the RLN directly. If a substantial decrease of EMG amplitude is observed after any test, the side of RLN experiment is complete, and EMG response will be continuously monitored for at least 20 min. (B) The SED is tested at a 5 mm distance close to the left RLN. (C) APS EMG signal when doing the activation study. Abbreviations: SED = surgical energy device, RLN = recurrent laryngeal nerve, EMG = electromyographic, APS = automatic periodic stimulation. Please click here to view a larger version of this figure.
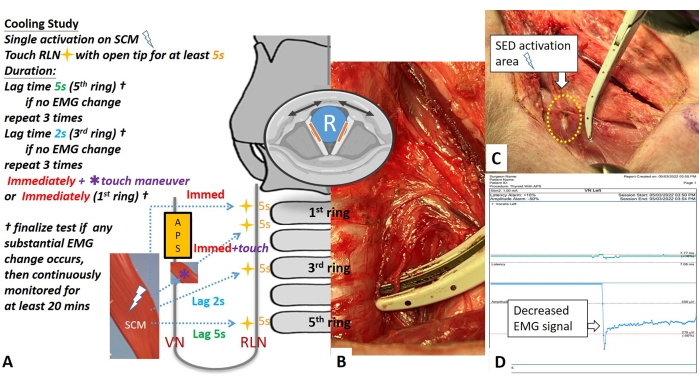
Figure 5: Flowchart of EP cooling study protocol. (A) The tests are performed on the RLN from the proximal (caudal) segments to the distal (cranial) segments. After the SED activation on the ipsilateral SCM muscle (white arrow) and after varying cooling times, touch the tip on the RLN (yellow star) for a 5 s period. If EMG response remained unchanged after three tests of 5 s cooling time, 2 s cooling time tests are performed. If the EMG response remained unchanged after repeated tests, final safety tests are performed by touching the SED tip with the RLN immediately after a single or double activations with or without the touch maneuver (asterisk). (B) The tip of the SED is opened to touch the inner noncoating part on the RLN. (C) The touch maneuver (asterisk) is quick touching/cooling with SCM after activation. (D) The APS EMG signal when doing the cooling study. Abbreviations: RLN = recurrent laryngeal nerve, SCM = sternocleidomastoid, EMG = electromyographic. Please click here to view a larger version of this figure.
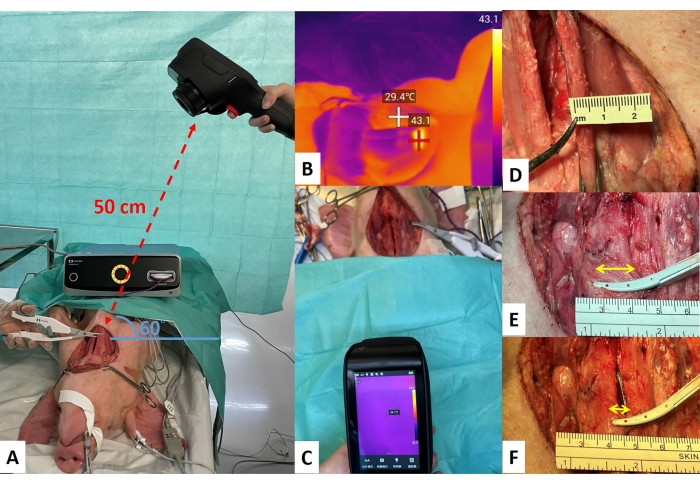
Figure 6: Thermal imaging system setting. (A) The camera was placed 50 cm from the target tissue and at an angle of 60° from the experimental table. (B) The operating field is measured by a thermal imaging camera. The temperature is displayed according to the color scale and the highest temperature on the screen is marked with a "+" sign. (C) Record the background temperature of the experimental area. (D) The standard strap muscle thickness for SED activation is 5 mm. (E) Whole blade test in a dry environment. (F) One-third (1/3) blade tests in a dry environment. Abbreviation: SED = surgical energy devices. Please click here to view a larger version of this figure.
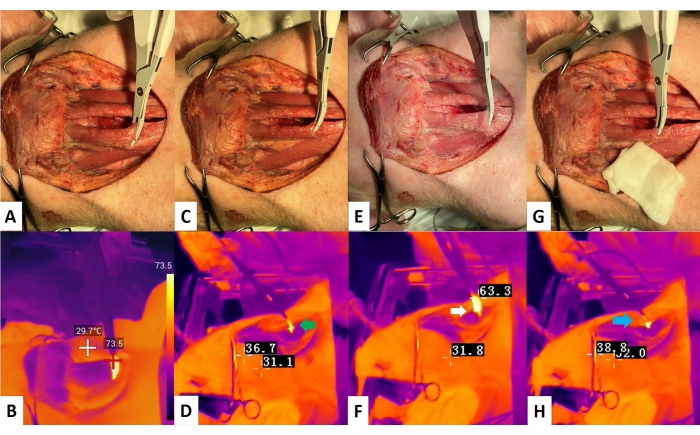
Figure 7: TG activation study. (A,B) A: Whole blade tests in a dry environment; B: TG image, the maximum activation temperature is more than 60 °C during the activation. (C,D) C: One-third (1/3) blade tests in a dry environment; D: TG image, splashing (green arrow) is observed after activation. (E) Whole blade tests in the wet environment; (F) TG image, more obvious lateral thermal spread is observed (white arrow) compared to the dry environment. (G) One-third (1/3) blade tests in a wet environment. (H) TG image, smoke (blue arrow) is more obvious compared to dry environment. Abbreviation: TG = thermographic. Please click here to view a larger version of this figure.
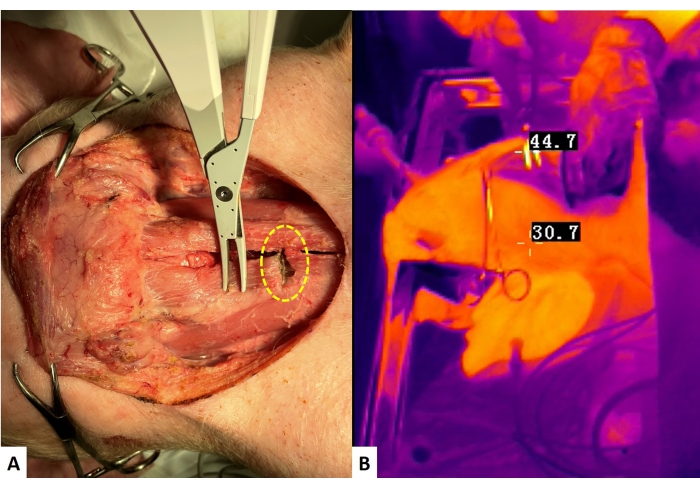
Figure 8: TG cooling study with MTM. (A) After a single activation of the SED with the whole blade on the strap muscle (yellow dotted line circle), quickly touching (approximately 1 s) the activated surface of the SED with another position of the strap muscle. (B) The TG image shows the SED temperature immediately after leaving the SED from the strap muscle with the blade open. When the temperature is more than 60 °C, start recording the cooling time until the highest temperature on the screen is less than 60 °C. Abbreviations: TG = thermographic, MTM = muscle tough maneuver, SED = surgical energy devices. Please click here to view a larger version of this figure.
| Nerve No. | 5 mm, | 2 mm, |
| amplitude status | amplitude status | |
| Nerve 1 | stable (3) | stable (3) |
| Nerve 2 | stable (3) | stable (3) |
| Nerve 3 | stable (3) | stable (3) |
| LOS, loss of signal; The number in brackets are the number of tests | ||
Table 1: Electrophysiological (EP) activation study. This is one of the EP activation study results. Every distance is examined three times until the EMG signal is decreased or lost. Every SED is checked with three nerves. This data is obtained using Device A (Table of Materials).
| No. nerve | 5 s, | 2 s, | Immediately without MTM, |
| amplitude status | amplitude status | amplitude status | |
| Nerve 1 | stable (3) | stable (3) | LOS (1) |
| Nerve 2 | stable (3) | stable (3) | 47% loss (2) |
| Nerve 3 | stable (3) | stable (3) | LOS (2) |
| MTM, muscle touch maneuver; LOS, loss of signal; The number in brackets are the number of tests | |||
Table 2: Electrophysiological (EP) cooling study. This is one of the EP cooling study results. Every distance is examined three times until the EMG signal is decreased or lost. In this experiment, the MTM are also examined. Every SED is checked with three nerves. This data is obtained using Device A (Table of Materials).
| Maximum activation temperature (°C) | |||||
| Blade | Test 1 | Test 2 | Test 4 | Test 5 | Maximum |
| Whole blade | 74.7 | 73.5 | 72.3 | 74.1 | 77.4 |
| Lateral thermal spread distance (in dry environment) (mm) | |||||
| Blade | Test 1 | Test 2 | Test 4 | Test 5 | Maximum |
| Whole blade | 3.7 | 5.2 | 4.9 | 4.2 | 5.3 |
| One-third blade | 4.2 | 4.7 | 4.5 | 5.0# | 5.2# |
| Lateral thermal spread distance (in wet environment) (mm) | |||||
| Blade | Test 1 | Test 2 | Test 4 | Test 5 | Maximum |
| Whole blade | 5.2*# | 4.3# | 6.7 | 4.6# | 6.7*# |
| One-third blade | 3.9*# | 4.5# | 5.1# | 5.7*# | 5.7*# |
| * with smoke; # with splashing | |||||
Table 3: Thermographic (TG) activation study. This is one of the TG activation study results. Every activation is examined five times under camera. This data is obtained using Device A (Table of Materials).
| Minimum cooling time (to 60 °C) without MTM (s) | ||||
| Test 1 | Test 2 | Test 3 | Test 4 | Test 5 |
| 6 | 5 | 5 | 6 | 6 |
| Blade Temperature after MTM (°C) | ||||
| Test 1 | Test 2 | Test 3 | Test 4 | Test 5 |
| 66.4 | 44.7 | 65.3 | 61.5 | 51.8 |
| Minimum cooling time (to 60 °C) with MTM (s) | ||||
| Test 1 | Test 2 | Test 3 | Test 4 | Test 5 |
| 2 | – | 2 | 1 | – |
Table 4: Thermographic (TG) cooling study. This is one of the TG cooling study results. Every activation is examined five times under camera and the cooling time is recorded. This data is obtained using Device A (Table of Materials).
| EP safety parameters | Device A |
| Activation distance | 2 mm |
| Cooling time | 2 $ s |
| TG safety parameters | Device A |
| Activation temperature @ | 77.4 °C |
| Lateral thermal spread distance | |
| Dry condition: whole blade (one-third blade) | 5.3 mm (5.2# mm) |
| Wet condition: whole blade (one-third blade) | 6.7 mm*# (5.7*# mm) |
| Cooling time | |
| without MTM | 6 s |
| with MTM (Blade temperature after MTM) | 2 s (66.4 °C) |
| $ No EMG signal loss after using MTM to cool the SEDs; @ with whole blade in dry environment; | |
| * with smoke; # with splashing; MTM, muscle touch maneuver | |
Table 5: Electrophysiological (EP) and Thermographic (TG) safety parameters. The table integrated the EP and TG safety parameters evaluated in this study. This data is obtained using Device A (Table of Materials).
