1. Create Silicone Molds for Tumor-simulating Inclusions
- Collect solid items of the desired shape and size that can serve as models for tumor-simulating inclusions, e.g., beads or marbles.
- Thoroughly clean the tumor models. To ensure an easy removal from the silicone mold, the tumor models can be sprayed with anti-stick spray or covered with a thin layer of petroleum jelly or beeswax.
- Place each model in a separate thin walled square (plastic) box with a smooth surface. If necessary, fixate the model to the bottom of the box to keep it in position. Use a box that is slightly bigger than the tumor model itself to avoid wasting excessive amounts of silicone.
- Pour the required amount of silicone component A in a mixing bowl and add silicone component B in a 10:1 ratio by weight. Mix both components thoroughly. Optionally, a vacuum pump can be used to remove air bubbles from the silicone mixture.
- Gently pour the silicone mixture in the plastic box to prevent trapping air bubbles. The silicone mixture should be processed within 45 min to obtain optimal results.
- Let the silicone mixture solidify for at least 6 hr before cutting the mold and removing the tumor model. Optionally, the silicone mold can be cut in a zigzag pattern to allow it to fit back together cleanly. Maximum strength of the silicone is obtained after 3 days.
2. Create Tris-buffered Saline Solution
- Create a Tris-buffered saline (TBS) solution by adding 6.1 g (50 mM) Tris and 8.8 g (150 mM) NaCl to 800 ml deionized water.
- Add 1.0 g (15 mmol) of NaN3 to block oxygenation of hemoglobin (step 3.3 and 4.4) and to inhibit bacterial growth. CAUTION: NaN3 is a severe poison. It may be fatal in contact with skin or if swallowed. The toxicity of this compound is comparable to that of soluble alkali cyanides and the lethal dose for an adult human is about 0.7 g. Always follow the safety instructions as provided by the manufacturer.
- Adjust the pH to 7.4 and bring the volume to 1,000 ml with deionized water.
3. Create Fluorescent Inclusions
- Add 2 g agarose to 50 ml TBS from step 2. The higher melting point of agarose compared to gelatin (step 4.2) will prevent the inclusions from dissolving and leaking fluorescent dye when placed in melted gelatin. Optionally, the amount of added agarose can be altered to 1 or 3 g to obtain softer or palpable tumor inclusions, respectively.
- Heat the agarose slurry using a microwave until the boiling point is reached. Stir thoroughly until the agarose is completely dissolved.
- Add 1.1 g (17 µmol) hemoglobin and 5 ml intralipid 20% dissolved in 50 ml of TBS to the agarose mixture under constant stirring to resemble the optical characteristics of the surrounding breast phantom tissue (step 4).
- Add 20.0 mg (25.8 µmol) of the fluorescent dye indocyanine green to 83.8 ml deionized water. Make sure the dye is completely dissolved.
- Pipet 5.0 ml from this solution and add it to the agarose mixture to obtain a final concentration of 14 µM. Optionally, other fluorescent dyes than ICG can be used if desired with their own optimum concentration.
- Gently fill the silicone molds created in step 1 with the hot agarose mixture using a syringe (Figure 1A). Repeat this process until all molds are filled.
- Let the fluorescent inclusions solidify at RT for approximately one hr. Protect the inclusions from light by covering the entire mold with aluminum foil.
- After solidification, gently open the mold and press out the inclusion (Figure 1B). Optionally, use the tip of the syringe to apply small drops of melted agarose mixture on the surface of the inclusion. By repeating this process several times on the same location, small tumor spurs can be created to simulate infiltrative tumors.
- Protect the agarose inclusions from light and dehydration by wrapping them in aluminum foil and store them in a humidified storage container at 4 °C.
NOTE: The use of lower or higher fluorescent dye concentrations than the known concentration optimum will both result in diminished fluorescent signal intensity. The seemingly counterintuitive reduction in signal intensity with increasing dye concentrations above the optimum fluorescent dye concentration is due to a phenomenon known as quenching. When assessing the maximal depth penetration of a fluorescent dye in phantoms, using the optimal concentration is mandatory.
4. Create Breast Phantoms
- Obtain a cup-shaped mold to create breast phantoms of the desired size and volume, e.g., a glass or plastic bowl. The mold should have a smooth surface to prevent the gelatin form adhering to the mold. A mold volume of 500 ml will create breast phantoms of sufficient size.
- To create a breast phantom with a volume of 500 ml, add 50 g of gelatin 250 bloom to 500 ml TBS (step 2). Heat the gelatin slurry to 50 °C under constant stirring.
- Once the gelatin is completely dissolved, let the gelatin mixture gradually cool down and maintain it at a constant temperature of 35 °C using a hot water bath.
- Under constant stirring, add 5.5 g (85 mmol) bovine hemoglobin and 25 ml intralipid 20% to simulate absorption and scattering of photons in tissue, respectively.
- Prechill the cup-shaped mold at 4 °C for at least 1 hr. Next, pour the gelatin mixture in the mold to a level that corresponds to the predefined depth of the agarose tumor-simulating inclusion (Figure 1C). Let the gelatin mixture solidify at 4 °C for 30 min to one hr.
- After solidification, position a tumor-simulating fluorescent agarose inclusion on the surface of the phantom and temporarily fixate the inclusion with a small needle. Up to a maximum of three tumor-simulating fluorescent inclusions can be incorporated in a single breast phantom. Sufficient space (at least 5 cm) should be kept between individual tumor-simulating inclusions (Figure 1D).
- Pour the remainder of the warm gelatin mixture in the remaining mold volume, allowing for adherence of both layers without creating refraction artifacts. Mark the location of the fluorescent tumor-simulating inclusions on the mold. Let the phantom solidify O/N at 4 °C.
- Once solidified, remove the needles used for temporary fixation of the inclusions and gently remove the breast phantom from its mold (Figure 1E). Protect the breast phantom from light and dehydration by wrapping it in aluminum foil and store it in a humidified storage container at 4 °C.

Figure 1. Sequential steps of creating breast phantoms containing fluorescent tumor-simulating inclusions. After creating silicone molds of the desired shape and size, the molds are filled with melted agarose mixture using a syringe (A). Tumor-simulating inclusions of differing size and shape were produced in the current study (B). Next, a thin layer of melted gelatin mixture is poured in a customized coated wooden breast mold (C). After solidification, the tumor-simulating inclusions are positioned, temporarily fixated, and covered with another layer of melted gelatin mixture (D). After solidification, the breast phantom is gently removed from its mold (E). The phantom can then be applied for simulating various NIRF imaging applications (F). Please click here to view a larger version of this figure.
5. Set the NIRF Camera System
- A NIRF camera system for intraoperative application is required for simulating targeted NIRF imaging in breast cancer surgery. Several NIRF imaging systems for real-time intraoperative NIRF imaging are currently available for investigational use. Although some differences between these devices exist, they all contain an excitation light source (for excitation of the fluorescent tumor inclusions) and a highly sensitive imaging device for detection of emitted photons.
- Make sure to use an excitation light source of a sufficient wavelength. For tumor-simulating inclusions containing ICG, use an excitation light source (e.g., laser) that emits photons between 750 and 800 nm. If an alternative fluorescent dye is used, the excitation wavelength should be adjusted conform the manufacturer’s instructions.
- In case the NIRF camera system contains an emission filter to filter out unwanted background signals, make sure that the correct filter is used. For tumor-simulating inclusions containing ICG, use an emission filter between 800 and 850 nm. Alternative fluorescent dyes may require different emission filters, depending on the manufacturers’ instructions.
NOTE: Make sure that there is zero overlap between the excitation and the emission wavelengths to prevent oversaturated images. In addition, the image acquisition time might have to be adjusted to obtain optimal fluorescent images. In the case of deep seated fluorescent inclusions or weak fluorescent signals, image acquisition time can be increased for up to several sec to min. In the case of superficial inclusions or strong fluorescent signals, acquisition time can be decreased to several msec to allow for video-rate fluorescence imaging in real-time.
6. Simulation of NIRF Imaging Applications in Breast Cancer Surgery
- Take the tissue-simulating breast phantom from its container and place it on a flat nonfluorescent surface. Next, position the NIRF imaging device above the breast phantom, leaving a sufficient working distance for excision of the tumor-simulating inclusions.
- Localize the tumor-simulating fluorescent inclusion using NIRF imaging and/or palpation of the phantom breast. In case no fluorescent signal can be detected, the inclusion is either positioned too deep in the phantom for detection or the image acquisition time should be increased.
- Once the inclusion is localized, incise the phantom breast and remove the tumor-simulating inclusion under real-time NIRF-guidance using conventional surgical instruments. Alternatively, the inclusion can be excised guided solely by visual inspection and palpation of the breast phantom to simulate the standard-of-care.
- Directly after removal of the tumor-simulating inclusion, image the surgical cavity for any remaining fluorescent activity indicating inadequate excision.
- In case of any remaining fluorescent activity, excise the inclusion remnant under direct NIRF guidance until no fluorescent signal is left.
- Image the excised phantom fragments to simulate NIRF-guided macroscopic margin status assessment. Hereto, slice the phantom tissue in 3 – 5 mm plaques and image the plaques accordingly. Fluorescence signal reaching into the surgical margins indicates the existence of positive surgical margins.
Results from this study have been previously reported elsewhere9.
Our data show that NIRF imaging can be applied to detect fluorescent tumor-simulating inclusions in tissue-simulating breast phantoms, simulating NIRF-guided breast-conserving surgery in breast cancer patients. Using our phantom model, we found intraoperative tumor localization, NIRF-guided tumor resection, intraoperative assessment of surgical cavity margins, and detection of residual disease to be feasible (Figure 2). In brief, a total of four phantom breasts were produced, all containing two fluorescent inclusions with distinct dimensions and/or morphology (Table 1).
Fluorescent tumor-simulating inclusions were removed surgically from the first and second breast phantom using conventional surgical instruments. Excision of the inclusions was guided by palpation and visual inspection of the operative field. The surgeon was asked to operate on the phantom breast until the tumor-simulating inclusions were completely removed. Next, the customized fluorescence camera was applied to scan the surgical cavity for any remaining fluorescent signals. In the case of an incomplete excision, indicated by a strong remaining fluorescence signal, the surgeon was requested to excise the inclusion remnant under real-time NIRF guidance. In both phantom #1 and #2, excision of one out of two tumor-simulating inclusions was incomplete, as evidenced by a strong remaining fluorescence signal originating from the surgical cavity. In the case of incomplete excision after the first surgical attempt, the surgeon detected and excised the remnant inclusion under NIRF guidance during the same (so-called theranostic) procedure. Reexcision under direct NIRF guidance resulted in a complete removal of the inclusion remnant at the second surgical attempt in all cases, while there was no need to excise large volumes of phantom tissue.
In the third and fourth breast phantom, NIRF-guided localization and surgical removal of the fluorescent inclusions was performed at the first surgical attempt. While approaching the tumor-simulating fluorescent inclusions, the surgeon had a monitor at his disposal on which the fluorescence signal was projected in real-time. In the fourth breast phantom, a tumor-simulating inclusion positioned at 3.0 cm depth was only detectable after incising the phantom tissue approximately 1 cm. In the third breast phantom, both tumor-simulating inclusions were radically removed at the first surgical attempt, whereas the removal of one infiltrative inclusion in the fourth phantom was found to be incomplete. Reexcision under direct NIRF-guidance resulted in a complete removal of the tumor remnant in this phantom.
Postoperatively, excised phantom tissue fragments were cut into 3 mm slides and imaged using the NIRF camera system to simulate ex vivo macroscopic evaluation of the surgical margin status. In all cases, postoperative NIRF imaging clearly depicted the borders of the tumor-simulating inclusions and indicated whether tumor-remnant was present at the surgical margins (Figure 2C).
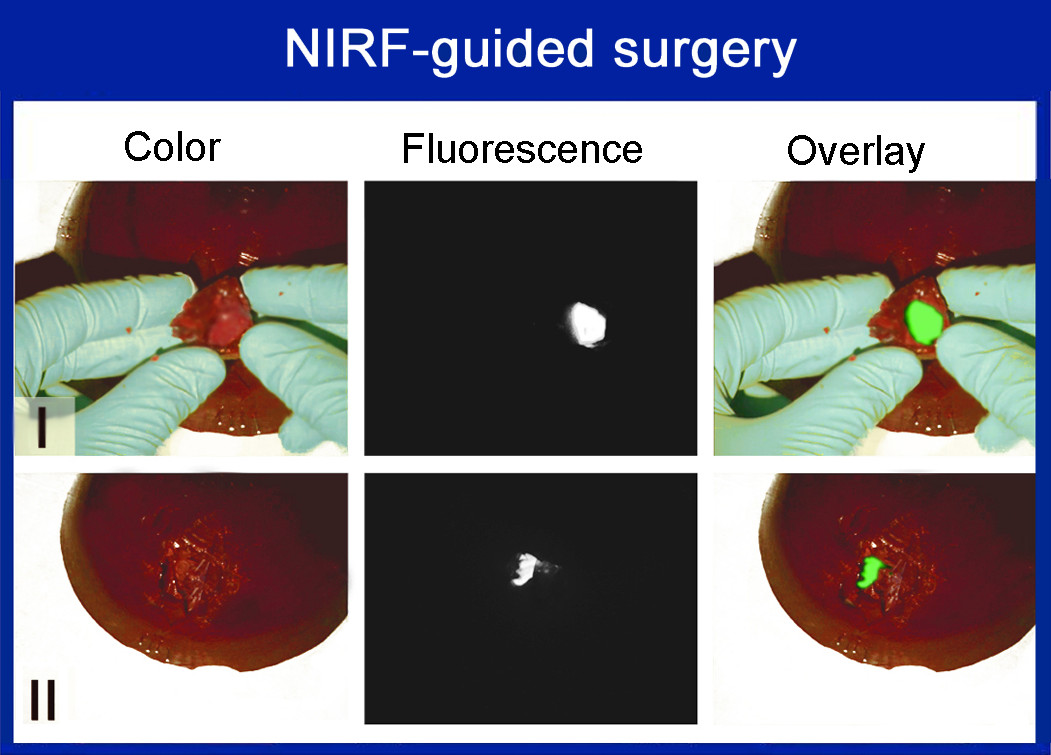
Figure 2. NIRF imaging simulation in breast phantoms. Tissue-simulating breast phantoms containing fluorescent tumor-simulating inclusions were applied for simulation of intraoperative tumor localization (A), NIRF-guided tumor removal (B), and NIRF-guided assessment of surgical margin status (C). Modified from: Pleijhuis et al., EJSO (2011). Please click here to view a larger version of this figure.
Table 1. Overview of phantom composition. 
A total of 4 phantoms were produced, containing two tumor-simulating fluorescent inclusions each of different size and shape.
