Figure 1B depicts classic Barrett’s Esophagus with no dysplasia surrounded on the borders by normal squamous epithelium. Beginning with the flatter squamous tissue, which is peripherally located and indicated by the blue arrows, a homogenous area of dull fluorescence is present with no glandular architecture. The green arrows indicate a circular green line surrounding the squamous tissue. This outline is artifact resulting from the cap of the endoscope. Moving to the centrally located Barrett’s tissue, glandular structures can be defined as green fluorescence surrounding a darker lumen. Although some glands are elongated, there is little distortion between adjacent glands, as the width of the glands is similar and the edges are clearly defined. Lastly, the glands and the lumens are evenly spaced with no clumping or crowding present.
Figure 2B depicts Barrett’s Esophagus with Low-Grade Dysplasia. It is important to note that although there is Low-Grade Dysplasia present, this cannot be visualized by morphological criteria via this imaging modality. Thus, based on morphological patterns, this tissue is still classified as benign. While the homogenous glands and lumens in the yellow oval are suggestive of mere metaplasia, the blue oval indicates an area of largely coalesced glands. That is, the thickness of the glands have increased, while the darker luminal cavity has become thin and nearly absent. These crowded and slightly distorted glands, however, have discrete, borders and tend to be homogenous. Moreover, there is no effacement present as the edges of the glands are smooth, thus the tissue is still benign. The red arrow indicates tissue that is out of focus and in video can be readily distinguished. Lastly, the black arrow shows bubbles that are artifact.
In Figure 3B, the red oval indicates the most prominent area with high grade dysplasia. These glands are crowded as they have thin irregular borders along with areas of tissue with near effacement of the glandular architecture. That is, the glands are no longer distinct, but rather fusing together, with their lumens being small and irregular. Although small, the continued presence of some lumens likely indicates high-grade dysplasia as it is more often in invasive cancer where the lumens are completely lost. In contrast to the high-grade dysplasia, the yellow oval highlights malignant tissue. Here, the glandular architecture is obliterated and lumens are largely absent.
Figure 4B depicts a centrally located adenocarcinoma. Notice first the cancer within the red oval and the complete obliteration of glandular architecture with luminal absence. This obliteration can be further appreciated when comparing the cancer to the tissue indicated by the blue arrow, which possesses some glandular framework. On the left, the gray rectangle highlights squamous epithelium, which can be better appreciated in video when the endoscope pans over it in its entirety. This squamous tissue is a flat homogenous area of dull fluorescence with no glandular architecture.
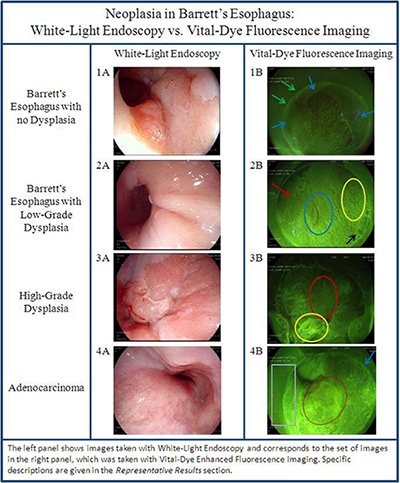
Figure 1. Neoplasia in Barrett’s Esophagus: White-light endoscopy vs. vital dye fluorescence imaging. (Left) Images taken with white-light endoscopy. (Right) Corresponding images taken with vital-dye enhanced fluorescence imaging. Please click here to view a larger version of this figure.
