Tubular injury and recovery may be assessed by H&E or PAS staining of tissue sections following renal IRI. Tubules located within the OSOM are classified as healthy, injured, necrotic or recovering according to cell morphology, integrity and nuclei number (Figure 1). The functional and structural injury in this model is dependent upon the duration of ischaemia. A progressive increase in the severity of renal dysfunction, assessed by plasma creatinine and BUN, is evident as the duration of ischaemia is increased by 2min increments (Figure 2). The extent of structural renal injury, inferred from the ATN score, follows a similar trend with more severe ATN accompanying more prolonged ischaemia (Figure 3). Following an initial titration of varying durations of ischaemia, this model of renal IRI should achieve a near 100% success rate, with all mice developing both functional and structural injury following surgery. This model of renal IRI also enables a fine level of control over the degree of injury with limited variation observed between animals (Figures 2 and 3). The use of different durations of ischaemia enables therapeutic interventions to be examined for their ability to modulate different levels of injury severity. For example on the basis of the length of ischaemia the resulting injury can be classed as mild (20 min), moderate (22 min) or high (24 min). These values are for male Balb/c mice aged 8 weeks and are included as guidance only. Investigators should establish their own experimental conditions as these will differ according to mouse strain, age, sex and the biochemical assay used to assess renal function.
This model has been successfully used to study regeneration following renal IRI with both renal function and structure recovering over the ensuing days. A gradual decline in plasma creatinine and BUN levels are observed, with plasma creatinine returning to basal levels by day 7 (Figure 4). An assessment of H&E stained tissue sections indicates that an increased number of tubules are classified as healthy or recovering at day 7 compared to day 4 indicating that tissue regeneration is taking place (Figure 5). The administration of 5-bromo-2'-deoxyuridine (BrdU) prior to sacrifice facilitates the immunostaining of kidney tissue for BrdU and subsequent quantification of tubular cell proliferation. Dramatic nuclear BrdU expression is observed 4 days following renal IRI indicating that the tubules are undergoing marked cell proliferation in order to restore tubule integrity and function (Figure 6). The combination of renal function assessment, scoring for structural improvement and BrdU immunostaining enables this model to be used to study regeneration following renal IRI. This allows the long-term effects of therapeutic interventions to be investigated.
Lastly, the utility of this model is dependent upon the induction of global ischaemia to the entire kidney and this may be jeopardized by the presence of blood vessels supplying the kidney in addition to the main left renal artery. If these additional vessels are not clamped then part of the kidney will not be subjected to ischaemic injury (Figure 7).

Figure 1. Scoring of structural tubular injury and regeneration – Representative morphology of healthy, recovering, injured and necrotic tubules. Tissue sections from a kidney removed 4 days following renal IRI are stained with PAS for assessment. Tubules located within the OSOM are classified as healthy, injured, necrotic or recovering according to cell morphology, integrity and nuclei number with representative examples highlighted. Healthy tubules are intact with a normal cellular morphology. Necrotic tubules exhibit a compromised monolayer with evident cell loss and loss of cell morphology. Injured tubules exhibit a thinned cellular monolayer and contain fewer nuclei. In contrast, recovering tubules exhibit a more normal cellular morphology and a similar number of nuclei to healthy tubules. Magnification: 400x. Please click here to view a larger version of this figure.
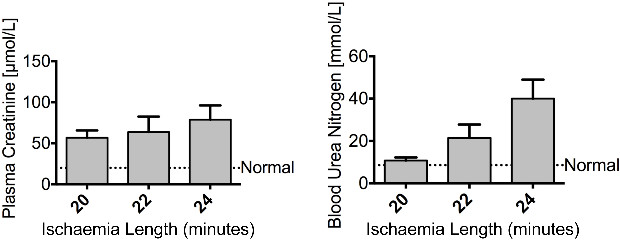
Figure 2. Injury – Renal ischaemia impairs renal function. Male Balb/c mice aged 8 weeks underwent a right nephrectomy and the left renal pedicle was clamped for 20, 22 or 24 min (n = 4 per group). Mice were sacrificed at 24 hr following renal IRI. Plasma creatinine and blood urea nitrogen show an increasing trend of severity as the length of ischaemia increased. The dashed line represents the levels of plasma creatinine and blood urea nitrogen found in normal control mice. Data presented as mean ± SEM and analyzed by one-way ANOVA. Please click here to view a larger version of this figure.
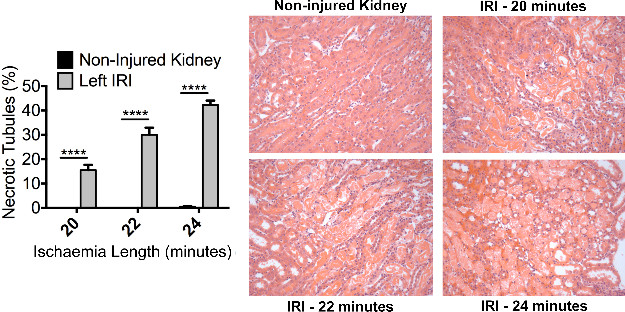
Figure 3. Injury – Renal ischaemia induces significant acute tubular necrosis. Male Balb/c mice aged 8 weeks underwent a right nephrectomy and the left renal pedicle was clamped for 20, 22 or 24 min (n = 4 per group). Mice were sacrificed at 24 hr following renal IRI. Representative photomicrographs (Magnification: 200x) of the OSOM from H&E stained kidney sections of control and injured kidneys illustrate ATN. Formal scoring of ATN (expressed as the proportion of necrotic tubules) confirms the increased level of injury with increasing duration of ischaemia. Data presented as mean ± SEM and analyzed by one-way ANOVA (**** = P ≤ 0.0001). Please click here to view a larger version of this figure.
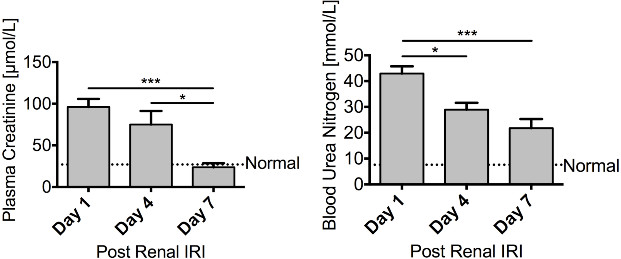
Figure 4. Regeneration – Renal function recovers following renal ischaemia. Male FVB mice aged 8 – 10 weeks underwent a right nephrectomy prior to 25 min of ischaemia to the left kidney. Mice were sacrificed 1 day (n = 10), 4 days (n = 10) or 7 days (n = 6) following renal IRI. Both plasma creatinine and blood urea nitrogen steadily decline over the course of 7 days, with plasma creatinine returning to basal levels, illustrating a recovery in renal function. Data presented as mean ± SEM and analyzed by one-way ANOVA (*** = P ≤ 0.001, * = P ≤ 0.05). Please click here to view a larger version of this figure.

Figure 5. Regeneration – Renal tissue shows signs of recovery following renal ischaemia. Male FVB mice aged 8 – 10 weeks underwent a right nephrectomy prior to 25 min of ischaemia to the left kidney. Mice were sacrificed 4 days (n = 10) or 7 days (n = 6) following renal IRI. Representative photomicrographs (Magnification: 200x) of the OSOM following the induction of ischaemia are shown. Formal scoring of the number of healthy, recovering, injured or necrotic tubules within the OSOM was assessed in PAS stained paraffin sections. At day 4 following renal IRI a large proportion of tubules within the OSOM still appear injured. However by 7 days there is a considerable increase in the proportion of tubules that are classified as healthy or recovering indicative of renal regeneration. Data presented as mean ± SEM. Please click here to view a larger version of this figure.
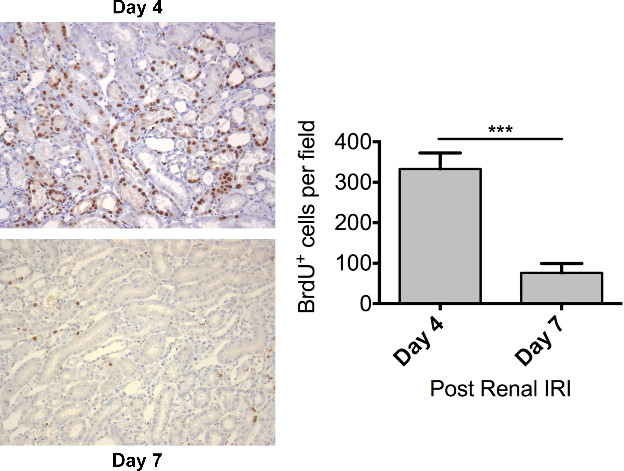
Figure 6. Regeneration – Dramatic tubular proliferation is evident 4 days following renal ischaemia. Male FVB mice aged 8 – 10 weeks underwent a right nephrectomy prior to 25 min of ischaemia to the left kidney. BrdU (50 mg/kg) was administered by intraperitoneal injection 24 hours prior to sacrifice. Mice were sacrificed 4 days (n = 10) or 7 days (n = 6) following renal IRI. Representative photomicrographs (Magnification: 200x) of the OSOM from mice sacrificed at day 4 and day 7 following the induction of ischaemia are shown. Tubular cell proliferation was assessed by immunohistochemical staining for BrdU on paraffin embedded kidney sections. Tubular cell proliferation was quantified by counting the number of BrdU positive nuclei in the OSOM with increased cell proliferation evident at day 4. Data presented as mean ± SEM and analyzed by students t-test (*** = P ≤ 0.001). Please click here to view a larger version of this figure.
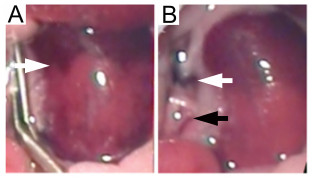
Figure 7. Left ischaemic kidney with non-occluded additional renal blood vessels. Failure to occlude additional blood vessels supplying the kidney leads to inconsistent ischaemia. (A) The absence of global kidney ischaemia is indicated by an uneven color change (white arrow) when the micro serrafine clip is in position. (B) Following removal of the micro serrafine clip, the main renal artery and vein are visible (white arrow) together with the additional blood vessel supplying the middle and lower pole of the kidney (black arrow). Please click here to view a larger version of this figure.
