Workflow for procuring and culturing sterile breast ductal carcinoma in situ tissue
Breast tissue sterility is maintained from the operating room to the cell culture lab via minor changes in typical hospital pathology workflow (Figure 1). Tissue is transported in a sterile container with a plastic film cover which allows radiologic assessment while maintaining tissue sterility. Gross tissue processing of a breast lumpectomy or mastectomy sample is performed with sterile gloves, blades, and tissue marking dyes. Gross morphologic appearance of breast ductal carcinoma in situ resembles pale, slightly raised areas with a gritty/firm texture, surrounded by reddish/yellow rubbery tissue. Areas of ductal hyperplasia and DCIS may feel “gritty” and firm due to calcifications. These areas of breast tissue often appear tan or a slightly different color than the surrounding breast tissue. However, ADH can only be distinguished after tissue collection and pathologic review of the stained tissue sections. Breast tissue remains viable by immersing the tissue and/or ductal organoids in serum-free nutrient medium supplemented with human recombinant EGF (10 ng/ml), insulin (10 μg/ml), streptomycin sulfate (100 μg/ml) and gentamicin sulfate (20 μg/ml)5. Cell culture flasks with removable/re-sealable lids permit periodic harvesting of cells/organoids (Figure 1E-F). This model successfully propagated human breast pre-invasive lesions from more than 20 patients diagnosed with atypical ductal hyperplasia (n = 2) and ductal carcinoma in situ (n = 18).
Spontaneous mammosphere formation in vitro and in vivo
Mammospheres and 3-D structures arose spontaneously from multiple, independent human DCIS duct tissue fragments from different patients diagnosed with atypical ductal hyperplasia or ductal carcinoma in situ (Figure 3 & 4)5,9. Enzymatic disruption of the breast tissue was not performed prior to tissue culture, which resulted in a mixed-cell type culture. Neither serum, basement membrane extract, nor gel-like matrices were required for spontaneous mammosphere formation (Figure 4). The mammospheres generated mammary xenograft tumors in a NOD/SCID mouse model with the same growth pattern as that of invasive cancer (Figure 5)5. These results demonstrate that progenitor cells with invasive potential pre-exist within the human breast DCIS duct but are apparently held in check by the ductal niche and can be coaxed to emerge in organoid culture. These cells constitute a new category of breast stem-like cells that exist prior to the overt manifestation of the invasive phenotype5,9,10.
Confirmation of epithelial derived mammospheres and xenografts
The mammospheres and xenografts derived from the mammospheres were confirmed by immunofluorescence as having epithelial origins. Epithelial cell adhesion molecule (EpCAM) is a membrane glycoprotein expressed on epithelial cells11. Immunofluorescence with a mouse monoclonal antibody reactive to human EpCAM (green) and a nuclear stain (DAPI, blue) showed EpCAM positive cells in the mammospheres in culture (Figure 6A) and the center of a NOD/SCID xenograft (Figure 6B).
Verification of intact basement membrane boundaries
The mammosphere forming, neoplastic epithelial cells in this culture system were derived from pre-invasive breast lesions that were devoid of frank invasion or microinvasion, as verified by independent pathologic analysis under standard of care histopathologic diagnosis. Multiple organoid structures from the same patient generated mammosphere forming colonies that proved to be tumorigenic. In addition, histopathologic examination of the tissue used for organoid culture revealed confluent intraductal lesions with intact basement membrane boundaries (Figure 7B)5. Thus it can be concluded that the spontaneous mammospheres formed in this culture system are derived only from pre-invasive neoplastic areas and are not a product of rare areas of microinvasion5.

Figure 1. Workflow for maintaining tissue sterility during radiological imaging and gross tissue dissection. (A) In the operating suite, breast tissue (lumpectomy sample shown) is placed in a sterile tray and covered with sterile plastic wrap. The tissue can be imaged directly in the plastic tray. (B) Tissue grossing to identify areas of DCIS. Single-use only tissue orientation dyes are painted onto the tissue surface using sterile cotton tipped swabs. Household distilled white vinegar is poured directly onto the tissue and blotted with sterile cotton gauze. (C & D) Breast tissue is transported to the tissue culture lab in nutrient rich medium supplemented with antibiotics. Tissue dissection, to isolate the areas of DCIS, is performed using sterile gloves and blades/scalpels/scissors. The DCIS tissue is cut into multiple organoids for culture. (E & F) In vitro culture of breast organoids. Human DCIS tissue is placed directly in tissue culture flasks with removable lids, without prior enzymatic digestion of the tissue. A minimal amount of serum-free culture medium supplemented with epidermal growth factor and insulin supports cellular growth while maintaining an air-liquid interface around the organoid. Please click here to view a larger version of this figure.

Figure 2. Illustration of gross tissue processing for breast DCIS tissue. The lumpectomy or mastectomy tissue is cut into thin sections by slicing the tissue vertically without cutting all the way through the specimen. This dissection method is often referred to as “bread loaf technique” since the cut tissue resembles a loaf of bread. The area(s) suspected of containing DCIS are cut out and sliced into 2 – 3 mm slices for diagnostic pathology and organoid culture.
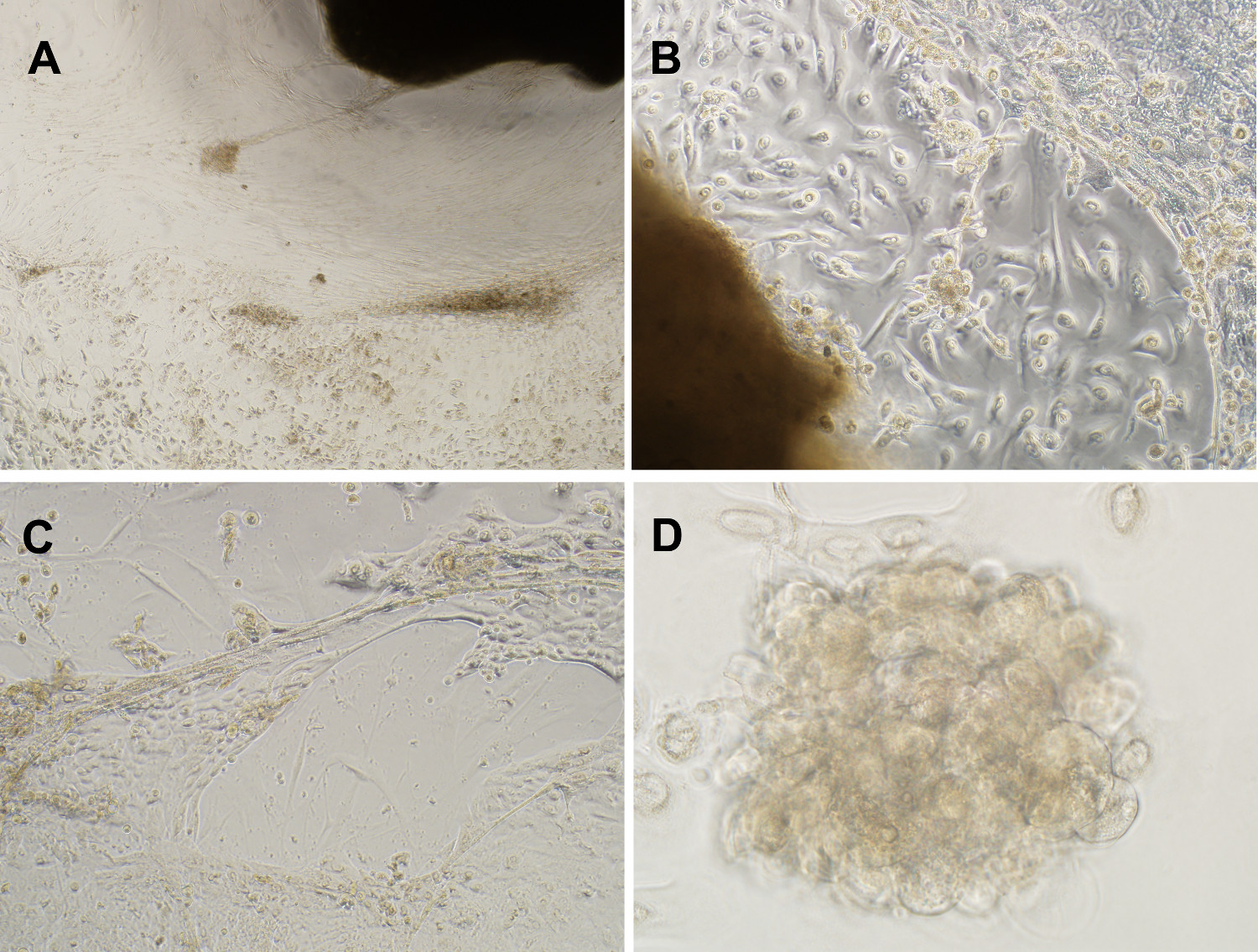
Figure 3. A mixed cell type culture maintains representative in vivo cell populations. (A) Phase contrast image of mixed cell culture generated from breast DCIS lesions over 11 weeks (4X magnification). (B & C) In vitro organoid cultivation successfully propagated DCIS derived epithelial cells with anchorage independent growth, defined as upward growing and expanding mammospheres, and lobulated, duct-like 3-D formations, in serum free medium supplemented with EGF, insulin, streptomycin and gentamicin (10X magnification). (D) Example mammosphere formed after 11 weeks in culture (40X magnification). Please click here to view a larger version of this figure.
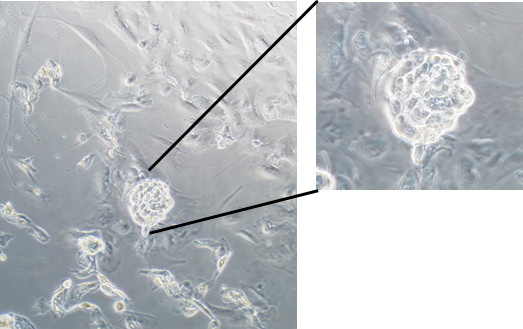
Figure 4. Spontaneous formation of mammospheres in serum free organoid culture. An example mammosphere formation following 33 days of culture (10X magnification, 20X inset). Please click here to view a larger version of this figure.
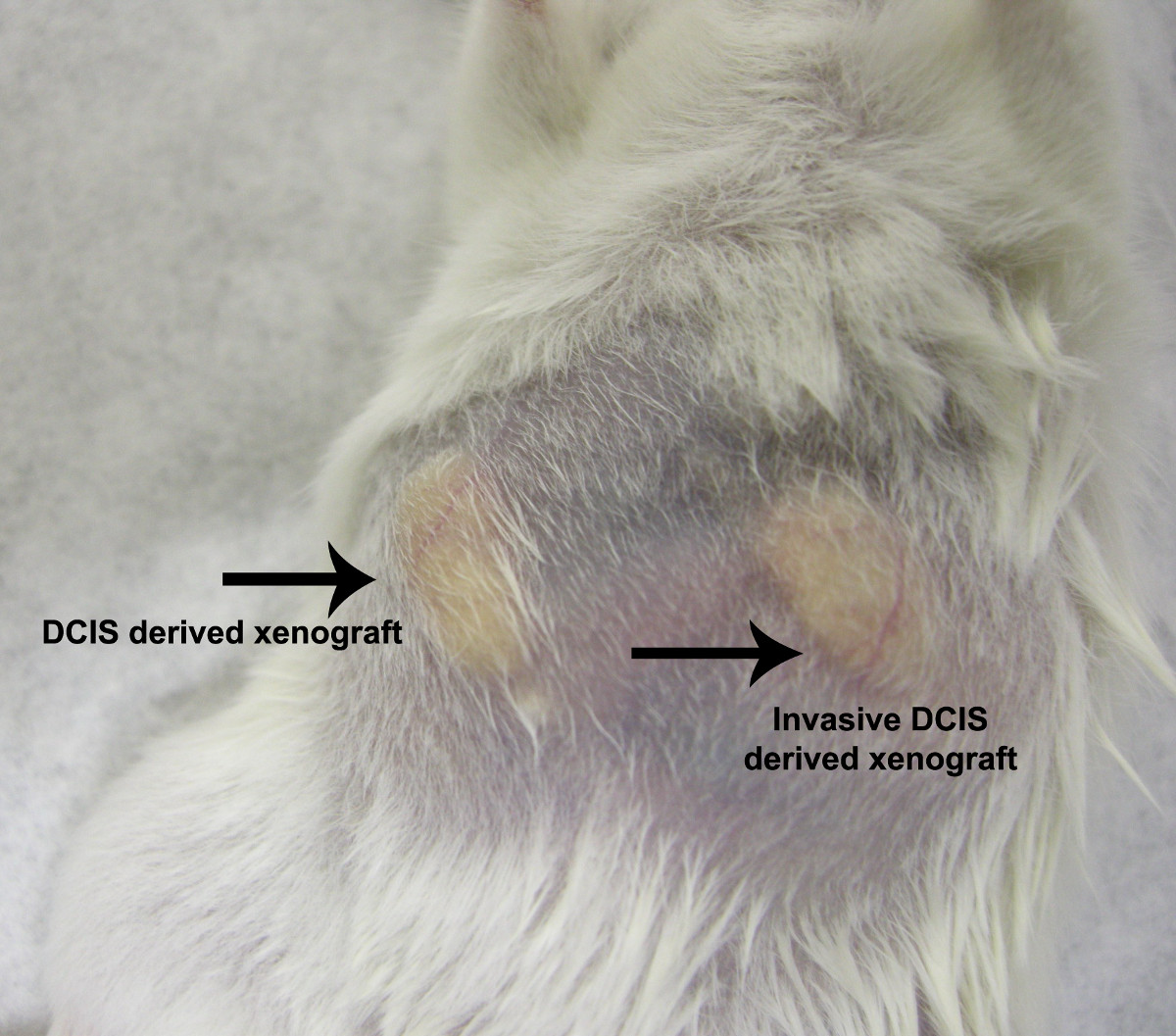
Figure 5. NOD/SCID mouse xenograft model. Xenografts were generated by injecting epithelial cells derived from a patient diagnosed with DCIS (mouse right mammary fat pad) or from a patient diagnosed with invasive DCIS (mouse left mammary fat pad). Xenografts derived from both pure DCIS and invasive DCIS revealed a similar growth pattern and rate. Please click here to view a larger version of this figure.

Figure 6. Mammospheres are confirmed to be of epithelial origin. Immunofluorescence with anti-EpCAM conjugated to FITC was used to confirm the epithelial origin of mammospheres and mouse xenografts generated from breast ducts containing DCIS. (A) EpCAM-FITC positive cells (pseudo-colored green, 488 nm) were only seen in mammospheres of the mixed cell cultures emanating from breast organoids (DAPI (pseudo-colored blue, 408 nm) nuclear stain). (B) In formalin fixed paraffin embedded mouse xenograft tissue sections, EpCAM positive cells were only detected in the center of the xenograft tumor section. (20X magnification) Please click here to view a larger version of this figure.
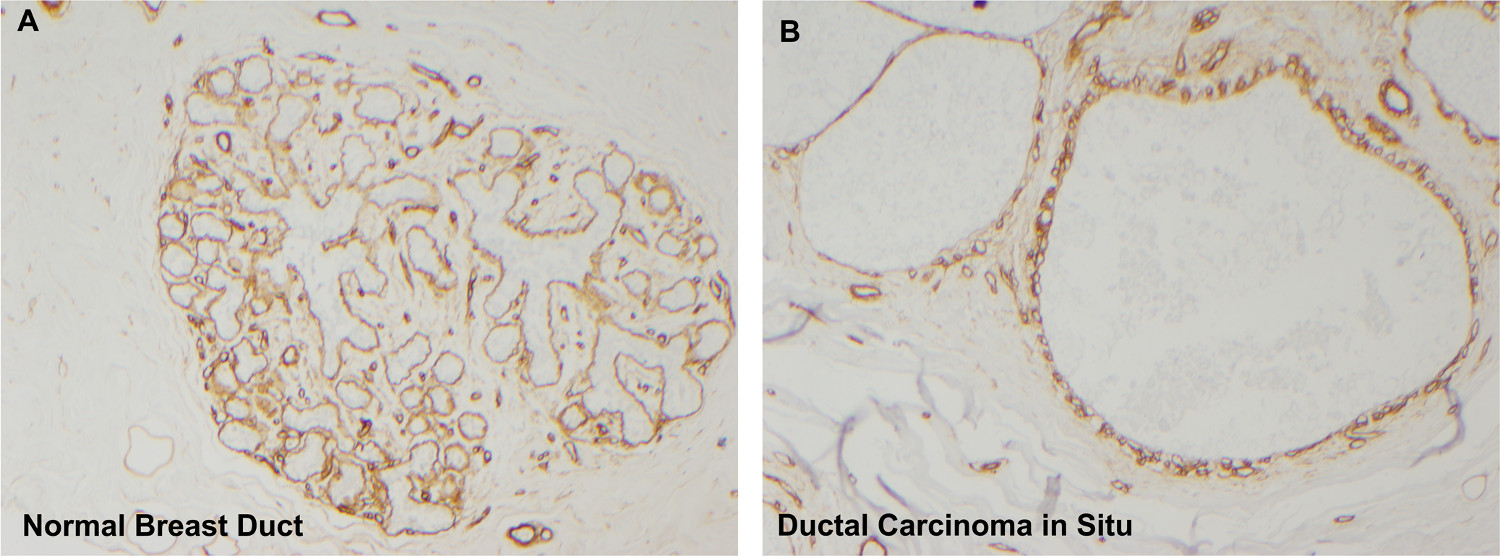
Figure 7. Collagen IV immunohistochemistry reveals intact basement membranes surrounding ducts. Normal breast ducts (A) are surrounded by intact basement membranes enriched in collagen IV (diaminobenzidine = brown staining). Following organoid culture, breast tissue also contains intact basement membranes confirming that the mammospheres are derived from areas of DCIS and not from invasive cancer (collagen IV immunohistochemistry, panel A 4X magnification, panel B 10X). Please click here to view a larger version of this figure.
