First, Muscle Energy Technique targets the Golgi tendon organs, which are stretch receptors located in skeletal muscle. Upon contraction, Golgi tendon organs are stretched, which activates afferent sensory type Ib nerves transmitting to the spinal cord. In the central nervous system, type Ib nerves synapse upon inhibitory motor neurons, which then provide inhibitory impulses to alpha motor neurons targeting the homonymous muscle group. The end result is relaxation of the initial and synergistic muscles, as well as contraction of antagonistic muscles. This effect is referred to as the Golgi tendon reflex or Inverse Myostatic Reflex. In the application of Muscle Energy Technique to the rib cage, muscles involved in breathing are engaged in isometric resistance. In the case of Rib 1, rib motion can be restricted by pathology related to the scalene muscles. By improving somatic dysfunctions in this respiratory muscle set, Rib 1 moves with greater ease during inspiration and expiration. Treatments that assist thoracic cage motion reduce the impedance of lymphatic flow by respiratory structures, which are located in the thoracic inlet/outlet area. Myofascial restrictions in clavicular region, such as scalene hypertrophy or spasm, can impede the terminal drainage of lymphatic vessels en route to the subclavian veins. Moreover, increased rib cage excursion improves pressure gradients, which further promotes lymph flow.
Second, Doming of the Thoracic Diaphragm Technique involves manipulation of the thoracic diaphragm, which is a principal muscle involved in breathing, blood circulation, lymphatic flow, and other key elements22. This technique involves “doming” the muscle to relieve hypertonicity associated with a flattened or dysfunctional state. Doming refers to the method of applying pressure and stretching the muscle in order to return it to a more normal rounded shape; thus, decreasing it’s hypertonicity. This technique indirectly engages the inferior surface of the diaphragm and increases its excursion during expiration26. Furthermore, the diaphragm assists lymphatic flow by exerting a pump-like propulsion effect on fluid within vessels. Thus, a hindrance in the diaphragm’s physical pumping force will limit lymphatic return to circulation. For instance, a hypertonic diaphragm can hamper the lymphatic flow from the cisterna chili, which is a major vessel that lies behind diaphragmatic attachments. The doming of the thoracic diaphragm technique increases excursion, and consequently there will be both optimal lymph flow and return pressure gradients to normal.
Third, Rib Raising Technique augments lymphatic flow by improving respiratory excursion and reducing sympathetic outflow. Excessive autonomic innervation reduces chest wall mobility by generating hypertonicity of the rib cage musculature and increasing intra-abdominal pressure27. Since lymphatic flow is dependent on pressure gradients generated by adequate respiratory excursion, excessive sympathetic tone can be a hindrance to lymphatic drainage28. Accordingly, this technique addresses this pathology by focusing on sympathetic chain ganglia adjacent to Ribs 2-626. Furthermore, in a study comparing the effect of Rib Raising to a light touch control group, there was a significant decrease in the levels of α-amylase, an established physiological biomarker of sympathetic activity29.
Fourth, Thoracic Pump Technique increases the flow of lymph and other immune cells through a rhythmic, phasic compression of lymphatic vessel walls and regional lymph tissue30, especially the thoracic duct. This technique provides a mechanical force to supplement lymphatic drainage into venous circulation, which is primarily useful in states of obstructed or limited drainage of the extracellular compartment. The oscillatory compressive action produces alternating pressure gradients, which enable lymph to flow through its natural channels in a superior direction.
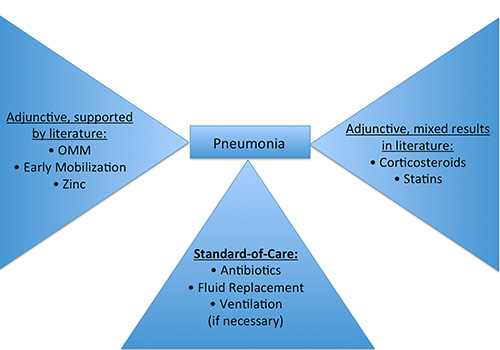
Figure 1. This figure illustrates various components of pneumonia treatment and their efficacy, as supported by current literature4.
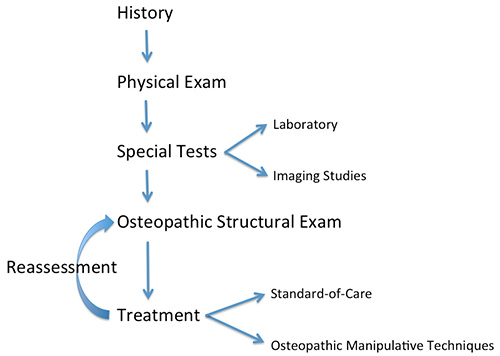
Figure 2. This figure illustrates the step-by-step approach toward patient care utilized by osteopathic physicians.
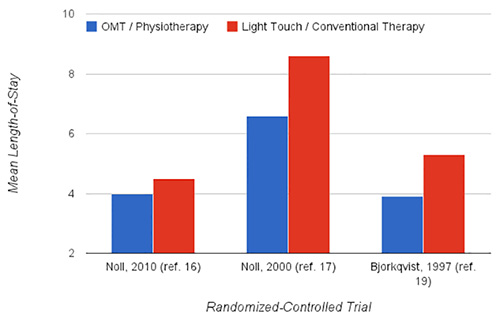
Figure 3. This figure demonstrates significant findings in RCTs comparing length of stay.
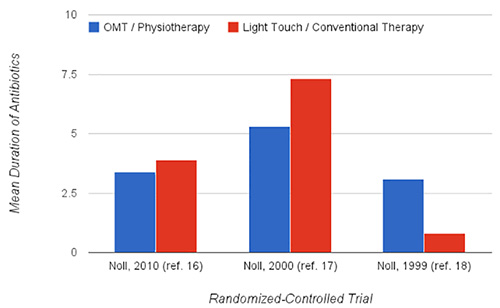
Figure 4. This figure demonstrates significant findings in RCTs comparing duration of antibiotics.
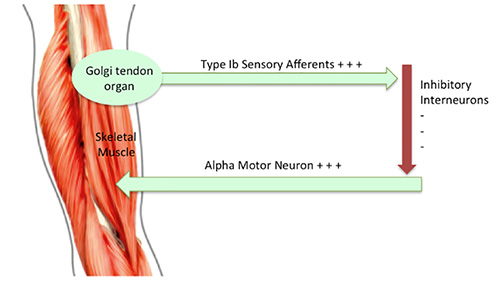
Figure 5. This figure demonstrates the Golgi tendon reflex. When stretched, the Golgi tendon organ is activated and provides feedback to the central nervous system that results in inhibitory impulses being sent to the homonymous muscle.

Figure 6. This figure demonstrates the positional set up for Muscle Energy Technique applied to an exhalation dysfunction of Rib 1.
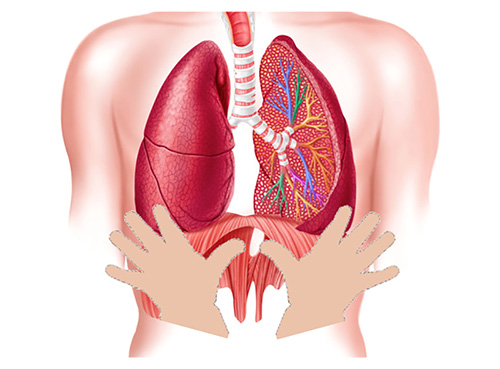
Figure 7. This figure illustrates placement of the thumbs for Doming the Diaphragm Technique, which normalizes the shape of the diaphragm to alleviate abnormal respiratory motions.

Figure 8. This figure demonstrates the positional set up for Doming The Diaphragm technique.
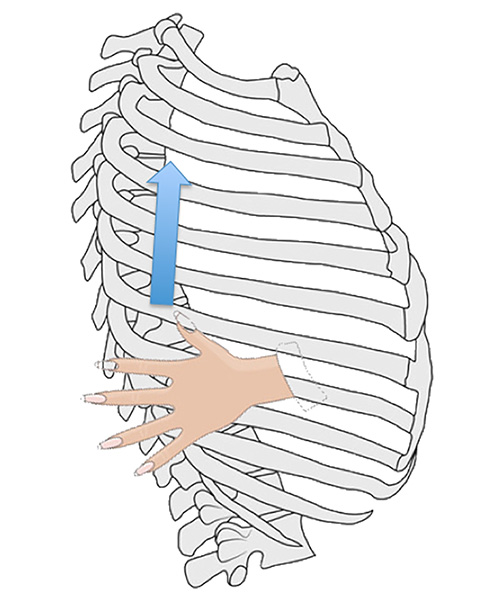
Figure 9. This figure illustrates the Rib Raising Technique, which improves respiratory expansion and alleviates hypertonicity caused by excessive innervation from the sympathetic chain ganglia.

Figure 10. This figure demonstrates the positional set up for Rib Raising Technique.
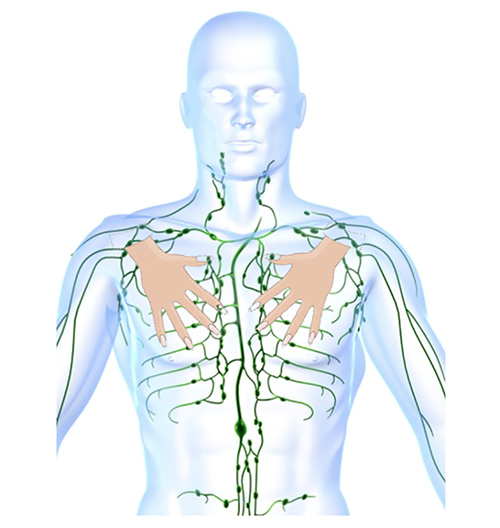
Figure 11. This figure illustrates hand positioning, relative to the lymphatic system, prior to providing downward oscillatory compression in Thoracic Pump Technique.

Figure 12. This figure demonstrates the positional set up for Thoracic Pump Technique.
