Figure 1A shows a schematic outlining the procedures detailed in this protocol summary. Several important factors must be considered for each step. For example, in Step 1 it shows two methods for sub-capsular tumor cell implantation into the kidney. Tumor cells can be implanted into the sub-capsular space with a small white-bubble confirming the localized placement of cells with leakage prevented by careful removal of needle and swabbing excess escaping fluid (Figure 1B-i). To prevent leakage, cells can be implanted internally first to reach the sub-capsular space (Figure 1B-ii), and combined with matrigel to prevent the initial distribution of tumor cells into the bloodstream. For surgical removal of kidney, exact timing depends on the growth and metastatic potential of the cell line used. Optimal nephrectomy practice includes a fast, but controlled, surgical procedure to minimize mouse distress and recovery. Tight and secure knotting of Vicryl to close ureter, renal artery and vein is key to avoid hemorrhaging (see Figure 1C). Cauterization should be used, but only if potential of excess bleeding requires intervention. Finally, tracking of spontaneous disease by non-invasive bioluminescent assessment allows continued monitoring of occult lesions and growth, as well as quantification at endpoint (see Figure 1D). However, the use of luciferase-labeled cells in spontaneous metastasis models can sometimes lead to clonal tumor cell selection of variants that may not express the transfected gene, and therefore may not always be visible after multiple rounds of selection or long-term tumor growth. In this case, clinically relevant histological analysis can be performed to identify micro-metastatic lesions or, if not technically (of financially) feasible, a visual scoring method to assess visual macro-metastatic disease can be used as a superficial measure of presence/absence of lesions in organ tissue (Figures 1D-i and 1D-ii).
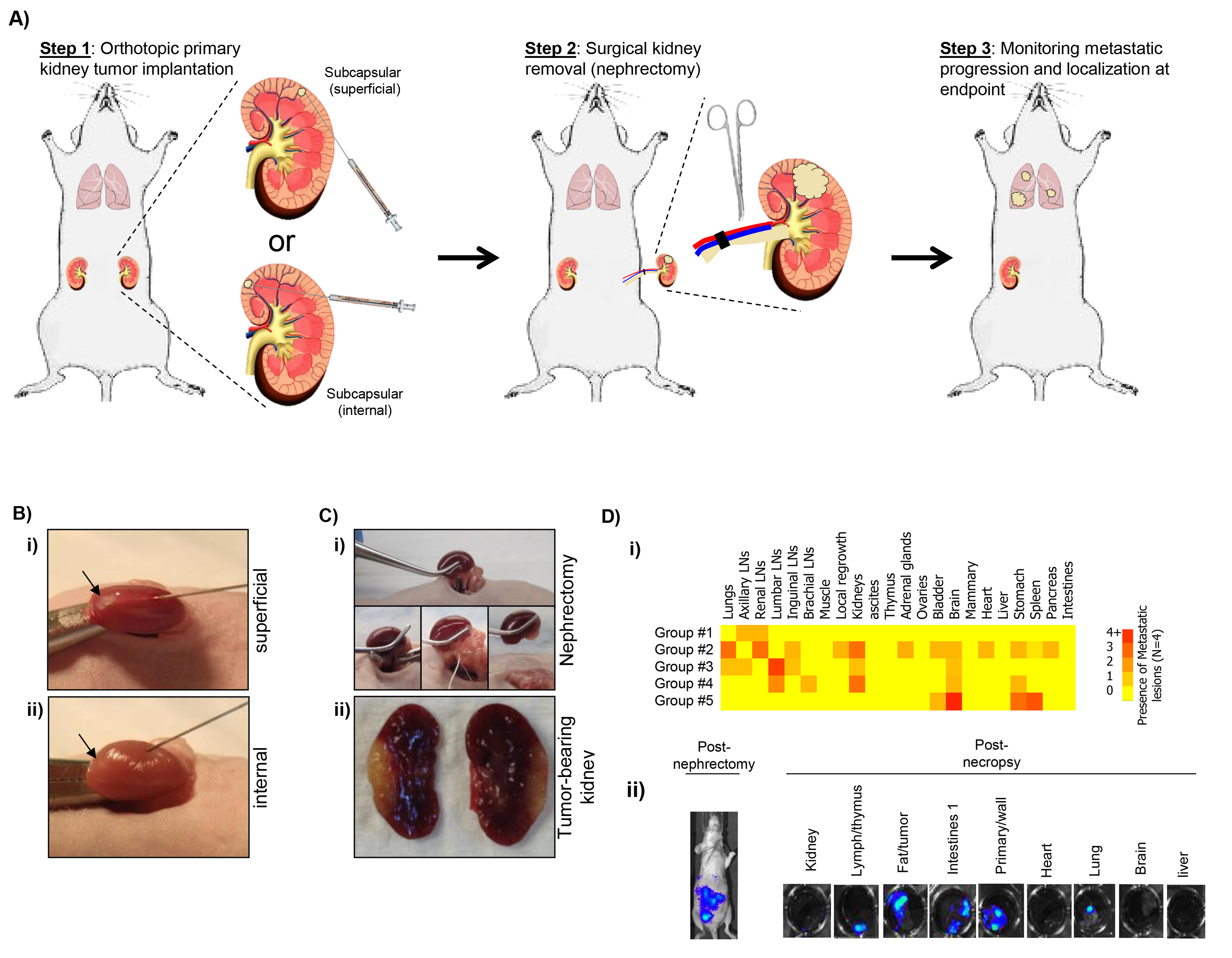
Figure 1. A) Schematic of surgical procedures including implantation (Step 1), surgical resection/nephrectomy (Step 2), and evaluation of post-surgical metastatic disease (Step 3). B) Example of sub-capsular implantation including (i) superficial and (ii) internal technique. C) Example of surgical nephrectomy procedure (i) and representative image of excised kidney with implanted tumor (ii). D) Assessment of post-surgical spontaneous metastatic disease using i) a visual scoring system to assess disease distribution (representative results from 5 groups of 4 animals), and ii) bioluminescent data immediately before and after sacrifice to quantitatively assess micro- and macro-metastatic lesions. Click here to view larger image.
