Summary
A novel methodology that is employed for the treatment of recurrent glioblastomas is described. This treatment approach employs the application of alternating electric tumor treating fields (TTFields), known as TTF Therapy in combination with bevacizumab, a targeted agent that is currently FDA approved as monotherapy.
Abstract
A novel device that employs TTF therapy has recently been developed and is currently in use for the treatment of recurrent glioblastoma (rGBM). It was FDA approved in April 2011 for the treatment of patients 22 years or older with rGBM. The device delivers alternating electric fields and is programmed to ensure maximal tumor cell kill1.
Glioblastoma is the most common type of glioma and has an estimated incidence of approximately 10,000 new cases per year in the United States alone2. This tumor is particularly resistant to treatment and is uniformly fatal especially in the recurrent setting3-5. Prior to the approval of the TTF System, the only FDA approved treatment for rGBM was bevacizumab6. Bevacizumab is a humanized monoclonal antibody targeted against the vascular endothelial growth factor (VEGF) protein that drives tumor angiogenesis7. By blocking the VEGF pathway, bevacizumab can result in a significant radiographic response (pseudoresponse), improve progression free survival and reduce corticosteroid requirements in rGBM patients8,9. Bevacizumab however failed to prolong overall survival in a recent phase III trial26. A pivotal phase III trial (EF-11) demonstrated comparable overall survival between physicians’ choice chemotherapy and TTF Therapy but better quality of life were observed in the TTF arm10.
There is currently an unmet need to develop novel approaches designed to prolong overall survival and/or improve quality of life in this unfortunate patient population. One appealing approach would be to combine the two currently approved treatment modalities namely bevacizumab and TTF Therapy. These two treatments are currently approved as monotherapy11,12, but their combination has never been evaluated in a clinical trial. We have developed an approach for combining those two treatment modalities and treated 2 rGBM patients. Here we describe a detailed methodology outlining this novel treatment protocol and present representative data from one of the treated patients.
Introduction
This novel TTF system is an FDA approved device that delivers intermediate frequency, low intensity alternating electric field directly to the brain for the treatment of recurrent glioblastomas1. It is considered a fourth treatment modality for the treatment of cancer in addition to surgery, radiation and chemotherapy. During preclinical experimentation, it was shown that the exposure of cancer cells to the tumor treating fields or TTFields resulted in disruption of cell division and subsequently apoptosis20.
Glioblastomas are the most common type of glioma and also the most aggressive. In the newly diagnosed setting, a standard treatment approach consists of concurrent radiation and temozolomide followed by adjuvant temozolomide for 6 months13. A recently completed phase III clinical trial showed a significant prolongation of median overall survival for patients treated with concurrent and adjuvant radiation with temozolomide as opposed to radiation alone. This trial led to the adoption of this protocol as a new standard of care for the management of newly diagnosed glioblastoma13. Unfortunately, those patients invariably relapse and treatment options become limited at that point. There is no standard approach for the treatment of recurrent glioblastoma; however, there are two FDA approved treatment modalities, namely bevacizumab and the novel TTF system. Bevacizumab, a monoclonal antibody directed against the VEGF protein results in the blockage of the VEGF protein/receptor interaction. This results in inhibition of vascular proliferation which is part of the tumor vasculature. The TTF system works through an entirely different mechanism, that is through delivery of continuous alternating electric fields that results in inhibition of cell division and apoptosis1,6,7,20. Despite all available treatment modalities, prognosis for recurrent glioblastoma remains dismal4.
Here we describe a novel approach for the treatment of recurrent glioblastoma using the delivery of both TTFields as well as the simultaneous bevacizumab infusion. The hope is that the combination approach would prove superior to monotherapy but this remains to be verified in a large scale clinical trial.
The Electromagnetic Basis for the TTF System
In order to understand the antimitotic effects of electric field-based treatment for GBM (Tumor Treating Fields therapy or TTF therapy), one must review a few concepts related to electromagnetic theory. This theory was formulated by Michael Faraday in the 1800s and states that a source charge is surrounded by an electromagnetic field18. This can exert a force on a test charge that is placed within that field. The electric field can be either uniform or non-uniform. In a uniform electric field, the field intensity remains uniform throughout. This can be represented by parallel lines of force. In a non-uniform electric field, the field intensity is non-uniform and varies from one end of the field to the other. This in turn can be represented by converging or diverging lines of force, where converging lines of force represent the area of higher field intensity and vice versa. A test charge will move towards the area of higher field intensity within that field. On the other hand, an electric field can either be constant or time-varying (alternating). The source charge in a constant electric field will remain the same while that same charge will oscillate/alternate between positive and negative in a time-varying field as a function of time19.
The direction of movement of a test charge in an electric field depends on several parameters. First, a test charge can be either an electric charge or a dipole. An electric charge is either positive or negative while a dipole is positive on one end and negative on the other. An electric charge will move towards the opposite charge while a dipole will rotate. The TTF System delivers an alternating electric field and therefore both charges and dipoles move or rotate in the direction of the opposite charge and higher field intensity. During the formation of the daughter cells in telophase, the morphology of the cells results in a non-uniform electric field and a field gradient leading to dielectrophoresis19. Dielectrophoresis is defined as the migration of uncharged particles towards the position of maximal field strength in a non-uniform field.
The Mechanism of the Anti-Mitotic Effects of Tumor Treating-Fields
The idea of using TTFields (tumor treating fields) for the treatment of cancer was originally conceptualized by Professor Yoram Palti20. Palti theorized that mitotic activity of cancer cells would be disrupted by applying properly tuned electric fields. The hypothesis was subsequently tested in various cancer cell cultures where it was demonstrated that electric fields disrupted the polymerization of tubulin subunits and therefore prevented the formation of mitotic spindles necessary for cell division20. For example, in an in vitro high-grade glioma model, the optimal TTField frequency shown to exert the maximal cell kill without excessive tissue stimulation or heating was determined to be 200 KHz20. The application of low frequency (<1 kHz) electric fields is known to result in biological tissue stimulation through membrane depolarization. As the frequency increases well above 1 kHz, the stimulatory effect greatly diminishes since the membranes hyperpolarization and depolarization cycles are integrated and the net effect becomes closer to nil. At significantly higher frequencies (MHz range), the electric fields result in tissue heating due to dielectric losses. This concept has been applied in clinical practice in applications such as diathermy and radiofrequency tumor ablation. The optimal effect was also dependent on the field intensity where fields in the rage of 1-3 V/cm were most effective without causing tissue heating. In addition, since the fields applied were of intermediate frequency (200 Khz in the case of glioma cells) they did not result in biological membrane stimulation. The application of low-intensity (1-3 V/cm), intermediate frequency (200 kHz) tumor treating fields to cells undergoing mitosis therefore resulted in the alignment of the highly charged tubulin subunits in the direction of higher field intensity, in this case towards the cells cleavage furrow. This resulted in disruption of mitosis, the formation of plasma membrane blebs and ultimately apoptotic cell death (see video portion of manuscript)20. Kirson and colleagues also showed that the maximal effects were observed when the field was applied roughly along the same direction as the cells undergoing mitosis. Fields applied in that manner and on a continuous basis for at least 24 hr were shown to result in arrest of cell proliferation and destruction of cells undergoing mitosis20. Using these preclinical data, the current method of applying the TTF System arrays is such that two sequential field directions are applied to the tumor to optimize cell kill rate. As such, the arrays layout is planned using the tumor MRI data to achieve the maximal desired biological activity.
Mechanism of Action of Bevacizumab and Rationale for Combining With Electric Fields for treating rGBM
Bevacizumab is a humanized monoclonal antibody that targets the VEGF molecule and prevents its interaction with the VEGF receptor. It received US Food and Drug Administration (FDA) approval in 2009 for the treatment of recurrent glioblastoma based on two phase II, open-label, non-comparative studies. In the BRAIN study, the objective response rate was 28% (24/85), with a median duration of response of 5.6 months. The PFS-6 rate with single-agent bevacizumab was 42.6% (95% CI, 29.6%–55.5%), and the median OS was 9.2 months (95% CI, 8.2–10.7 months)8. The second study (NCI 06-C-0064E) the objective response rate was 19.6% (11/56; 95% CI, 10.9%–31.3%). The median PFS was 16 weeks (95% CI, 12–26 weeks), the PFS-6 rate was 29% (95% CI, 18%–48%), and the median OS was 31 weeks (95% CI, 21–54 weeks)21. In summary, the two studies found that when compared with historical controls, the use of bevacizumab was associated with higher progression-free survival rates and disease response rates. On the other hand, there is no strong evidence to indicate that bevacizumab can prolong median overall survival when used as an upfront treatment for newly diagnosed GBM patients. Bevacizumab had been tried in combination with several chemotherapeutic agents in the past. A retrospective review of recurrent GBM patients treated with a bevacizumab containing regimen and subsequently treated with a different bevacizumab containing regimen after progression concluded that there is no benefit with continuation of bevacizumab following tumor progression27. Furthermore, despite the favorable radiographic response based on reduction in the enhancing disease seen after bevacizumab treatment, a recent study concluded that non-enhancing disease progression is common after bevacizumab treatment and may be associated with worse outcomes.28
Several preclinical and early clinical data indicate that the combination of tumor treating fields with chemotherapeutic agents maybe more effective (and potentially synergistic) than chemotherapy alone22,23,24. For example, a study assessed the effects of TTFields alone or in combination with various chemotherapies (paclitaxel, doxorubicin, cyclophosphamide and dacarbazine) on human breast carcinoma (MDA-MB-231) and human glioma (U-118) cell lines24. The same study examined the effects of TTFields in combination with these chemotherapeutic agents in an animal tumor model and in a pilot clinical trial in recurrent and newly diagnosed GBM patients. The study concluded that the sensitivity to chemotherapeutic treatment was increased by 1-3 orders of magnitude by the addition of TTFields. In a pilot clinical trial involving patients with newly-diagnosed and recurrent GBM, the combination approach resulted in a significantly improved PFS and OS (progression free survival of 155 weeks and overall survival of 39+ months) compared with historical controls26.
On the other hand, a large phase III trial comparing TTF Therapy to physicians’ choice chemotherapy in the treatment of rGBM (EF-11) showed that both treatment approaches resulted in similar survival outcomes while TTF Therapy afforded a better side effect profile compared with chemotherapy10. Given that both bevacizumab and TTF Therapy have shown activity and are currently FDA approved albeit as monotherapy for rGBM, we hypothesized that the combination of the two treatment modalities may afford an advantage over the use of either agent alone. One hypothesis of why the combination bevacizumab with chemotherapy may offer little advantage in terms of patient overall survival is the dependence of chemotherapy on compromise of the blood brain barrier. When bevacizumab corrects the blood brain barrier, it also affects the ability of chemotherapy to reach the tumor effectively. TTF Therapy as a physical modality is hypothesized not to be dependent on the blood brain barrier for it efficacy. There are limitations to utilizing this novel treatment approach. On the one hand, patient selection can be difficult especially given the contraindications for each treatment modality. It is unclear whether the contraindications for the combination approach are similarly those of the individual treatment modalities when employed as monotherapy or if there are additional precautions with the combination approach. From our limited experience with this novel approach, patients tolerated the treatment well. On the other hand, it remains to be seen in a large scale clinical trial whether this approach will provide any additional advantage (overall survival or progression-free survival) over the currently available treatment protocols. Currently, there is a large unmet need for developing effective treatment approaches for rGBM as its prognosis remains dismal despite all available treatment modalities. This approach will need to be assessed in a large scale clinical trial to determine if it can address this unmet need for this unfortunate patient population.
Protocol
NOTE: This protocol consists of two parts: the detailed methodology for applying the TTF System and the methodology for bevacizumab infusion8-11. The FDA mandates that only prescribers trained by the manufacturer may prescribe the device. Patients eligible for TTF Therapy are those 22 years of age or older with recurrent glioblastoma, typically after surgical, surgery and radiation options have been exhausted but should have received at least one prior chemotherapy regimen. Contraindications to the use of TTF Therapy include sensitivity to conductive hydrogels, the presence of an active implanted medical device (deep brain stimulators, spinal cord stimulators, vagus nerve stimulators, pacemakers, defibrillators, and programmable shunts), a skull defect or bullet fragment(s). While the TTF Therapy is generally well tolerated, the most typical device-related adverse event is skin redness and occasionally skin breakdown due to the prolonged contact of the transducer arrays to the skin surface. To minimize this potential side effect, the arrays are typically changed twice a week and if a skin reaction is observed, the arrays can be moved away from the site of skin redness or inflammation. These skin reactions can also be treated by topical steroids and/or topical antibiotics if needed1.
1. Application of the TTF System
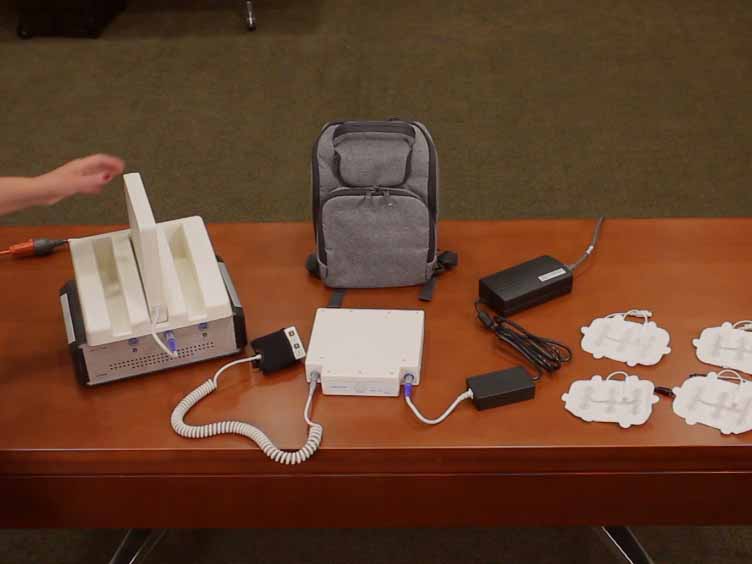
NOTE: the system consists of the following components: an electric field generator (the Device), a connection cable and box, a portable battery(s), a charger for portable batteries, a plug-in power supply, and a set of Transducer arrays (4) (Figure 1).
- Assembling the System
NOTE: In order for the electric field generator to deliver the electric fields to the tumor mass, the components have to be interconnected in the following manner:- Charge the battery(s) using the battery charger by connecting its power cord to a standard wall outlet and switch on the power button on the back of the charger.
NOTE: A battery rack can hold up to 3 batteries at a time. - Use a charged battery to power the electric field generator or “Device”, which in turn delivers the electric fields to the transducer arrays.
- Plug the battery in through its connecter to a socket labeled “DC IN” on the front panel of the device. Ensure that the arrows on the battery connector are facing up towards the “DC IN” sign while plugging in the connector.
- Turn on the power button after the battery is plugged into the device.
- Connect each of the four transducer array connectors, using the color coded plugs, to the matching color-coded socket on the connection cable box.
NOTE: for example, the transducer array connector with the red ring is plugged into the red socket (labeled “N1”) on the connection cable box (see Figure 1). - Connect the coiled connection cable to the box on one end and the device to the other end.
- Connect the battery to the device to provide the necessary power for the device to generate the alternating electric fields.
- Connect the device to the connection cable and box using the color coded sockets that match color coded cables attached to the transducer arrays.
- Charge the battery(s) using the battery charger by connecting its power cord to a standard wall outlet and switch on the power button on the back of the charger.
- Applying the Transducer Arrays to the Scalp
- Prepare the patients head for array application. Shave the entire scalp using an electric shaver. Ensure no stubble remains and wipe the scalp with 70% medical grade alcohol.
NOTE: An over-the-counter hydrocortisone (steroid) cream may be used if the scalp is irritated. - Lay out the transducer arrays according to a pre-determined specific array layout on a patients clean and shaven scalp.
NOTE: The array layout is calculated using special software that utilizes head and tumor measurements from the patients’ magnetic resonance imaging (MRI) in order to generate the optimal electric field intensity at the site of the tumor to achieve maximal results. - Peel off the envelopes and remove the arrays then apply to the scalp according to specific array layout color scheme.
NOTE: The transducer array locations and colors are: front (blue), back (red), right (yellow), left (white) according to where they are placed on the scalp.
NOTE: Transducer arrays are supplied in clear sterile envelopes. - Snap the plugs into the connector.
- Place the color-coded plugs on the transducer array connectors of the four transducer arrays.
NOTE: These colors match the color coding of the transducer array placement diagram that has been generated for each patient with the help of special software (1.2.2). - Plug the array cables into the color-matched connection cable and box as mentioned above (see section 1.1).
- Turn on the power switch on the device once the arrays are in place and the system is fully connected.
- Switch on the TTF Field button and the system is now ready for electric field delivery.
NOTE: There is no standard duration for continuation of TTF Therapy, however, in the author’s opinion TTF Therapy can be continued until the time of clinical and/or radiographic progression of the disease or development of unacceptable toxicity. To achieve an optimal response, TTF Therapy should be used on a continuous basis for a minimum of 18 hr a day. Treatment duration of less than 18 hr per day has been associated with suboptimal response. A monthly compliance log can be downloaded from the device software by a Novocure technician.
- Prepare the patients head for array application. Shave the entire scalp using an electric shaver. Ensure no stubble remains and wipe the scalp with 70% medical grade alcohol.
2. Concurrent Bevacizumab Administration
NOTE: Bevacizumab is a humanized monoclonal antibody targeted against the vascular endothelial growth factor (VEGF) protein. By blocking the interaction of VEGF with its receptor, bevacizumab exerts a potent anti-angiogenic effect6,7. Typically bevacizumab is administered as an IV infusion (typically over 30 min) every 2 weeks. However, the TTF device is designed to be used on a continuous basis or at least for 18 hr per day in order to achieve optimal outcomes10.
- Select patients carefully in order to minimize the potential for serious drug related complications.
NOTE: The exclusion criteria for bevacizumab include recent intracranial hemorrhage, recent stroke or MI (less than 1 year), major surgery within 4 weeks, uncontrolled hypertension, pregnancy or lactation and imaging showing minimal or no contrast enhancing disease. Also, caution must be exercised in patients with renal disease including proteinuria, bleeding disorders, history of DVT, uncontrolled angina, cardiac arrhythmias, congestive heart failure, prior chest wall radiation, prior anthracycline exposure, patients on anticoagulants, recent (less than 6 months) arterial thromboembolic events and other serious medical illness. - Prescreen patients with baseline testing to include complete blood count with differential, renal and liver function testing, serum electrolytes, urine dipstick for protein and pre and post infusion blood pressure measurement.
- Administer the bevacizumab infusion once a patient is deemed an appropriate candidate using the standard dose of 10 mg/kg body weight and start the TTF System simultaneously with the bevacizumab infusion.
NOTE: Give the initial infusion over 60 min and mix in 100 ml of normal saline. Provided that no complications develop, bevacizumab can be given over 30 min on subsequent infusions.
3. Monitoring Patients Post Infusion
- Monitor the patient for infusion reactions such as fever, chills, pruritis, rash or angioedema. If these occur stop the bevacizumab infusion, and treat the reactions using standard approaches based on their degree of severity8,9,11.
NOTE: Other complications of bevacizumab treatment that require dose modification or discontinuation include proteinuria and hypertension, both of which have been observed in clinical trials with bevacizumab8,9,11. - If acute hypertension (a rise of 20 mmHg or more in diastolic blood pressure or a blood pressure of 150/100 mmHg above normal baseline values) occurs, withhold bevacizumab. If the blood pressure subsequently returns to normal within 1h following the holding of the infusion, restart the infusion at ½ the initial rate. If sustained hypertension occurs then hypertension modification agents such as calcium channel blockers, ACE inhibitors or diuretics (hydrochlorothiazide).
- If proteinuria (2+, 3+ or 4+ on urine dipstick) occurs then perform a 24 hr urine collection for protein. If the 24 hr urine protein reveals a protein level of less than 2 g/24 hr then administer bevacizumab at full strength. For levels between 2-4 g/24 hr, administer bevacizumab at 5 mg/Kg body weight (½ the standard dose). Discontinue Bevacizumab for protein levels of more than 4 g/24 hr.
- Perform gadolinium-DTPA enhanced magnetic resonance imaging once every 8-12 weeks to assess for tumor response.
NOTE: A FLAIR sequence is also particularly helpful especially while administering bevacizumab, since occasionally the contrast enhanced component may diminish while the FLAIR signal change may show signs of progression. - Assess the radiographic change of the glioblastoma using the newly published Revised Assessment in NeuroOncology (RANO) criteria (modified from the older Macdonald criteria)16.
Representative Results
The above protocol was used to treat 2 patients with recurrent glioblastoma who have failed conventional surgical, radiation and chemotherapy treatments. Data obtained from one of those patients is discussed. Patient was a 56 year old female who was initially treated with standard chemo-radiation according to the “Stupp protocol”13. At the time of disease progression, she elected to pursue dose-dense temozolomide according to the protocol used in the previously reported “Rescue Study”14. Her disease remained stable for several months on dose dense temozolomide but subsequently developed a second radiographic progression in addition to myelosuppression (grade 3 thrombocytopenia). She then decided to pursue the above protocol with the knowledge that the combination approach represents an off-label use of bevacizumab and NovoTTF Therapy, since both are FDA approved as monotherapy in the recurrent setting. The patient continued with this combination approach for approximately 1 month. She was using TTF Therapy on average 10-12 hr a day but later became progressively agitated and was pulling on the device cables. The patient’s family then elected to discontinue therapy and pursue hospice care.
On follow up imaging, the tumor showed a significant radiographic response. Interestingly, both the enhancing (as represented by the MR post-gadolinium) and the non-enhancing disease (MR FLAIR sequence) showed radiographic regression (see Figure 2). When Avastin is administered as monotherapy for recurrent GBM, it is not unusual to observe a reduction in the enhancing component of the tumor while simultaneously observing progression of the FLAIR signal change. The exact mechanism underlying this tumor response is unclear however it is postulated that bevacizumab through reducing blood vessel “leakiness” and permeability may result in a decrease in gadolinium extravasation without affecting the non-enhancing disease15. Whether this combination approach resulted in a true reduction of both the enhancing and non enhancing components of the tumor remains to be verified in future large scale studies. Unfortunately, the patient expired approximately 2 months following initiation of this protocol. Patient had developed chest pain and shortness of breath (per her daughter's account) immediately prior to her death and therefore (although not proven through investigations) we felt that the cause of death was a catastrophic pulmonary embolus rather than directly related to her underlying GBM. As noted earlier, bevacizumab treatment is associated with an increased risk of pulmonary embolism6,11.

Figure 1: The NovoTTF-100A System components and assembly. (A) The transducer arrays are shown as they are applied to the scalp (1) with the array cables connected to the color coded sockets on the connection cable and box (2). The box in turn is connected to the electric field generator with the battery as the power supply (3). (B) Transducer arrays showing ceramic discs and connector.

Figure 2: Radiographic response of recurrent GBM to concurrent NovoTTF Therapy and bevacizumab. Pretreatment axial MR image post gadolinium-DTPA administration (a), coronal post gadolinium-DTPA (b), and FLAIR (c) in a 57 year old female with recurrent GBM. Post-treatment MR scans (1 month after concurrent treatment) showing significant reduction of both enhancing, axial (d) and coronal (e) as well as no-enhancing (f) FLAIR signal change.
Discussion
This article describes a novel approach for treating recurrent glioblastoma. The approach involves combining the only two FDA approved treatment modalities for recurrent disease. This involves the use of continuous low intensity, intermediate frequency electric field treatment with the TTF system in combination with the antiangiogenic agent, bevacizumab. Although each of those treatment modalities is FDA approved as monotherapy, given the dismal prognosis of GBM at the time of recurrence, combination approaches may prove superior to monotherapy, but this remains a subject of ongoing clinical trials. This approach has never been reported in the literature, however a clinical trial is currently examining whether this combination would result in better median overall survival in patients who relapsed after standard chemoradiation17.
Troubleshooting:
Several problems may potentially arise during the operation of the TTF device. For example, the device power indicator light may fail to switch on despite turning 'ON' the device. Possible reasons may include a dead battery, malfunctioning battery, charger or device. The first step would be to replace the dead battery with a fully charged spare. Otherwise, the device should be turned 'OFF' and the technical support helpline contacted. A cable may be detached from the transducer arrays, its connection cable or the device itself. This may indicate too much physical force on the cable or may indicate a faulty connection with the system components. Replacing the transducer arrays may fix the problem but if problem not fixed then once again the TTF therapy should be switched 'OFF' and the manufacturer contacted. The device also has a built in alarm system that indicates a problem with the device or its mode of operation. If the device alarm is activated this may indicate a low battery, loose or disconnected cable, blockage of the device side vents, poor transducer array contact or simply device malfunction. Troubleshooting should therefore include replacing the battery (especially if the low battery lights are lit), or if low battery lights are not lit then all connections should be checked to ensure there are no loose connections, side vents should be checked for blockages and transducer arrays also should be checked to ensure they are properly applied as well. If problem persists then again manufacturer should be contacted. Side effects from the application of the transducer arrays to the scalp may also arise and include itching, redness or less commonly blisters. In case of itching or redness, a 0.1% hydrocortisone cream may be applied and the arrays shifted by ¾ of an inch away from the site of itching or redness. Blisters on the other hand may indicate an infection and may require antibiotic treatment.
Limitations of the Technique:
The TTF system has been recently approved by the FDA for the treatment of recurrent GBM in patients 22 years and older. There are several contraindications for the use of the device. Those include use of an implanted device such as a deep brain or spinal cord or vagus nerve stimulators, programmable shunts, defibrillators and pacemaker devices. Also, the use of the TTF system is contraindicated in patients with a skull defect and/or bullet fragments. Sensitivity to conductive hydrogels such as those used with electroencephalogram stickers is a contraindication for use.
Apart from the rather limited scope for use, the application of alternating electric fields is not a known cure for recurrent GBM although the 2- and 3-year survival rates rates were 8% (95% CI: 4%–13%) and 4% (95% CI: 1%–8%) versus 5% (95% CI, 3%–10%) and 1% (95% CI, 0%–3%), for TTF versus active control.10 Its use has been shown to be equivalent to physicians’ choice chemotherapy but with lesser side effects after failure of standard approaches such as surgery radiation and first line chemotherapy regimens. As the therapy continues to be refined in the future, alternating electric fields may prove efficacious in the front line treatment of glioblastoma.
Significance with respect to existing methods:
As noted above, the TTF therapy is currently FDA approved for recurrent GBM and not for the front-line treatment for newly diagnosed GBM. The standard of care for the treatment of newly diagnosed GBM currently is the “Stupp” protocol, which involves the administration of concurrent radiation (60 Gy over 6 weeks) together with temozolomide chemotherapy followed by adjuvant temozolomide. Despite the significant prolongation of median overall survival of this treatment regimen, GBM is still a highly resistant disease to all forms of available treatment modalities and remains uniformly fatal. The addition of a fourth treatment modality, namely the alternating electric fields to the armamentarium for the treatment of GBM is much needed at this point. Future studies using a variety of combinations and permutations of TTF therapy with the other currently approved treatment modalities may prove highly beneficial.
Critical steps within the protocol:
The proper operation of the TTF system is critical for successful treatment. The steps described in the protocol section should be followed accurately but it should be noted that the FDA mandates appropriate training through the device manufacturer for healthcare providers who intend to use the device. The critical steps include charging the battery appropriately, assembling the components correctly as noted in the protocol section, properly shaving and cleaning the scalp, applying conductive hydrogel and finally applying the transducer arrays per the treatment layout to the shaved scalp. This helps ensure the proper conduction of the alternating electric fields to their intended brain region. After ensuring proper assembly of the TTF system and application of transducer arrays, the power button is turned ON and finally the TTField button is turned on to start treatment.
Future Directions:
The use of TTF therapy in the treatment of GBM, both in the recurrent and newly-diagnosed setting is likely to be refined in the future. Future studies with TTF therapy especially in the newly diagnosed setting maybe especially promising. Because of its unique mechanism of action and favorable safety profile, it is likely that TTF therapy in combination with a variety of chemotherapeutic as well as molecularly-targeted agents will be employed in future clinical trials. Currently there is an ongoing trial testing the safety and efficacy of TTF therapy in combination with adjuvant temozolomide in patients 18 years and older with newly diagnosed GBM (EF-14)25. A positive outcome from this trial may result in widening the indication of TTF therapy to include newly diagnosed GBM patients. In addition, the TTF therapy will also be tested for a variety of other cancers including metastatic brain disease. Hopefully, as the techniques are refined, these approaches will have a significant impact on such a uniformly fatal disease.
Disclosures
This study was supported by a grant from Novocure Limited to cover the publication costs.
Acknowledgments
We wish to acknowledge Dr. Angela Davies for her insightful comments during the preparation of this manuscript.
Materials
| Name | Company | Catalog Number | Comments |
| NovoTTF-100A System | Novocure Limited | Portsmouth, NH | |
| Bevacizumab (Avastin) | Genetech Corporation | South San Francisco, USA |
References
- Federal Drug Administration NovoTTF-100A system approval order and device summary. , (1000).
- CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in. , 2004-2008 (2012).
- Tanaka, S. Diagnostic and therapeutic avenues for glioblastoma: no longer a dead end. Nat Rev Clin Onco. 10, 14-26 (2013).
- Omar, A. I., Mason, W. P. Temozolomide: The evidence for its therapeutic efficacy in malignant astrocytomas. Core Evidence. 4, 93-111 (2010).
- Adamson, C. Glioblastoma multiforme: a review of where we have been and where we are going. Expert Opin Investig Drugs. 18, 1061-1083 (2009).
- Rinne, M. L. Update on bevacizumab and other angiogenesis inhibitors for brain cancer. Expert Opin Emerg Drugs. 18, 137-153 (2013).
- Jain, R. K. Tumor angiogenesis and accessibility: role of vascular endothelial growth factor. Semin Oncol. 29, 3-9 (2002).
- Friedman, H. S. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol. 27, 4733-4740 (2009).
- Vredenburgh, J. J. Bevacizumab plus irinotecan in recurrent glioblastoma multiforme. J Clin Oncol. 25, 4772-474729 (2007).
- Stupp, R. NovoTTF-100A versus physician's choice chemotherapy in recurrent glioblastoma: a randomised phase III trial of a novel treatment modality. Eur J Cancer. 48, 2192-2202 (2012).
- Cohen, M. H., Shen, Y. L., Keegan, P., Pazdur, R. FDA Drug Approval Summary: Bevacizumab (AVASTIN®) as Treatment of Recurrent Glioblastoma Multiforme. Oncologist. 14, 1131-1138 (2009).
- Davies, A. M., Weinberg, U., Palti, Y. Tumor treating fields: a new frontier in cancer therapy. Ann N Y Acad Sci. 1291, 86-95 (2013).
- Stupp, R. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 352, 987-9896 (2005).
- Perry, J. R. Phase II trial of continuous dose-intense temozolomide in recurrent malignant glioma: RESCUE study. J Clin Oncol. 28, 2051-2057 (2010).
- Takano, S. Decrease in the apparent diffusion coefficient in peritumoral edema for the assessment of recurrent glioblastomatreated by bevacizumab. Acta Neurochir Suppl. , 118-185 (2013).
- Wen, P. Y. Updated response assessment criteria high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol. 28, 1963-1972 (2010).
- NovoCure Ltd.. NovoTTF-100A With Bevacizumab (Avastin) in Patients With Recurrent Glioblastoma. , National Cancer Institute (NCI). Case Comprehensive Cancer Center. (2014).
- Faraday, M.
- Kirson, E. D. Alternating electric fields arrest cell proliferation in animal tumor models and human brain tumors. Proc Natl Acad Sci U S A. 104, 10152-107 (2007).
- Kirson, E. D. Disruption of cancer cell replication by alternating electric fields. Cancer Res. 64, 3288-3295 (2004).
- Kreisl, T. N. Phase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastoma. J Clin Oncol. 27, 740-745 (2009).
- Pless, M. A phase I/II trial of Tumor Treating Fields (TTFields) therapy in combination with pemetrexed for advanced non-small cell lung cancer. Lung Cancer. 81, 445-450 (2013).
- Schneiderman, R. S., Shmueli, E., Kirson, E. D., Palti, Y. TTFields alone and in combination with chemotherapeutic agents effectively reduce the viability of MDR cell sub-lines that over-express ABC transporters. BMC Cancer. 10, (2010).
- Kirson, E. D. Chemotherapeutic treatment efficacy and sensitivity are increased by adjuvant alternating electric fields (TTFields). BMC Med Phys. 9, 1-13 (2009).
- Gilbert, M. R. A Randomized Trial of Bevacizumab for Newly Diagnosed Glioblastoma. NEJM. 370, 699-708 (2014).
- Lee, E. Q. Role of a second chemotherapy in recurrent malignant glioma patients who progress on bevacizumab. Neuro Oncol. 11, 550-555 (2009).
- Iwamoto, F. M. Patterns of relapse and prognosis after bevacizumab failure in recurrent glioblastoma. Neurology. 73, 1200-1206 (2009).