Fonte: Alexander Goldfarb, MD, Assistente Professore di Medicina, Beth Israel Deaconess Medical Center, MA
Le malattie gastrointestinali rappresentano milioni di visite in ufficio e ricoveri ospedalieri ogni anno. L’esame fisico dell’addome è uno strumento cruciale nella diagnosi delle malattie del tratto gastrointestinale; inoltre, può aiutare a identificare i processi patologici nei sistemi cardiovascolari, urinari e di altro livello. Come esame fisico in generale, l’esame della regione addominale è importante per stabilire il contatto medico-paziente, per raggiungere la diagnosi preliminare e selezionare i successivi test di laboratorio e di imaging e determinare l’urgenza delle cure.
Come con le altre parti di un esame fisico, l’ispezione visiva e l’auscultazione dell’addome vengono eseguite in modo sistematico in modo che non vengano persi potenziali risultati. Particolare attenzione dovrebbe essere prestata a potenziali problemi già identificati dalla storia del paziente. Qui assumiamo che il paziente sia già stato identificato e abbia avuto una storia presa, sintomi discussi e aree di potenziale preoccupazione identificate. In questo video non esamineremo la storia del paziente; invece, andremo direttamente all’esame fisico.
Prima di arrivare all’esame, esaminiamo brevemente i punti di riferimento della superficie della regione addominale, dell’anatomia addominale e della topografia. Ecco un elenco di punti di riferimento utili: margini costali, processo xifoide, muscolo addominale retto, linea alba, ombelico, cresta iliaca, legamento inguinale e sinfisi pubica. L’esame addominale copre l’area in basso dai margini xifoidi e costali in modo superiore alla sinfisi pubica inferiormente.
Per scopi diagnostici e descrittivi, l’addome è suddiviso in quattro quadranti: quadrante superiore destro (spesso designato come RUQ), quadrante superiore sinistro (LUQ), quadrante inferiore destro (RLQ) e quadrante inferiore sinistro (LLQ)(Figura 1). La topografia più dettagliata dell’addome lo divide in 9 regioni: ipocondriaca destra e sinistra, lombare destra e sinistra, iliaca destra e sinistra, e anche regioni epigastriche, ombelicali e ipogastriche nel mezzo (Figura 2).
Ricorda quali organi in genere proiettano in ogni regione addominale (Figura 3). È essenziale conoscere bene l’anatomia e la topografia della regione per documentare e interpretare adeguatamente i reclami e i sintomi di un paziente, nonché i risultati fisici durante l’esame.
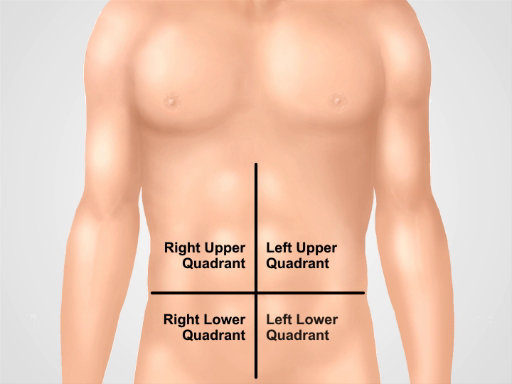
Figura 1. Quattro quadranti addominali. L’addome può essere diviso in quattro regioni da due linee immaginarie che si intersecano all’ombelico: vengono mostrati il quadrante superiore destro (spesso designato come RUQ), il quadrante superiore sinistro (LUQ), il quadrante inferiore destro (RLQ) e il quadrante inferiore sinistro (LLQ).
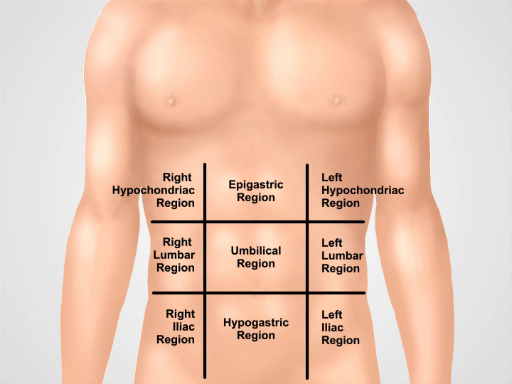
Figura 2. Nove regioni addominali. Le linee midclavicolari e i piani subcostali e intertubercolari separano l’addome in nove regioni: regione epigastrica, regione ipocondriaca destra, regione ipocondriaca sinistra, regione ombelicale, regione lombare destra, regione lombare sinistra, regione ipogastrica, regione inguinale destra e regione inguinale sinistra. I termini per le regioni epigastriche, ombelicali, ipogastriche e sovrapubiche sono i più comunemente usati nella pratica clinica.
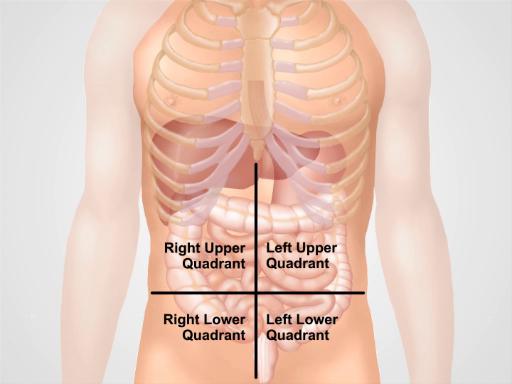
Figura 3. Posizione di diversi organi nelle quattro regioni addominali. Organi nella cavità addominale e la loro posizione rispetto a quattro quadranti addominali.