Fuente: Alexander Goldfarb, MD, profesor de medicina, centro médico Beth Israel Deaconess, MA
Enfermedad gastrointestinal representa millones de consultas y hospitalizaciones cada año. El examen físico del abdomen es una herramienta fundamental en el diagnóstico de enfermedades del tracto gastrointestinal; Además, puede ayudar a identificar procesos patológicos en los sistemas Cardiovasculars, urinarios y otros. Como el examen físico en general, el examen de la región abdominal es importante para establecer contacto médico-paciente, para alcanzar el diagnóstico preliminar y selección de laboratorio posteriores y pruebas de imagen y determinar la urgencia de la atención.
Como con el resto del examen físico, inspección visual y la auscultación del abdomen se realizan de manera sistemática para que le falten ningunos resultados potenciales. Debería prestarse atención especial a problemas ya identificados por la historia del paciente. Aquí suponemos que el paciente ya ha sido identificado y tenía tomado de la historia, síntomas discutidos y áreas de preocupación potencial identificado. En este video no revisaremos la historia del paciente; en cambio, nos dirigiremos directamente a la exploración física.
Antes de llegar al examen, vamos a repasar brevemente superficie lugares de interés de la región abdominal, abdominal anatomía y topografía. Aquí está una lista de puntos de referencia útiles: márgenes costales, proceso del xiphoid, músculo abdominal recto, linea alba, ombligo, cresta ilíaca, ligamento inguinal y sínfisis púbica. El examen abdominal cubre el área abajo de los márgenes de xiphoid y costales superior de la sínfisis púbica inferiorly.
Para propósitos de diagnóstico y descriptivos, el abdomen se subdivide en cuatro cuadrantes: cuadrante superior derecho (a menudo señalado como en CSD), a la izquierda del cuadrante superior (LUQ), cuadrante inferior derecho (CID) y cuadrante inferior izquierdo (CII) (figura 1). La topografía detallada del abdomen divide en 9 regiones: hipocondríaca derecha e izquierda lumbar derecha e izquierda, derecha e izquierda ilíaca y también las regiones epigástricas y umbilicales hipogástricas en el medio (figura 2).
Recordar que los órganos típicamente del proyecto en cada región abdominal ()figura 3). Es esencial conocer la anatomía y topografía bien adecuadamente documentar e interpretar un paciente quejas y síntomas, así como los resultados físicos durante el examen.
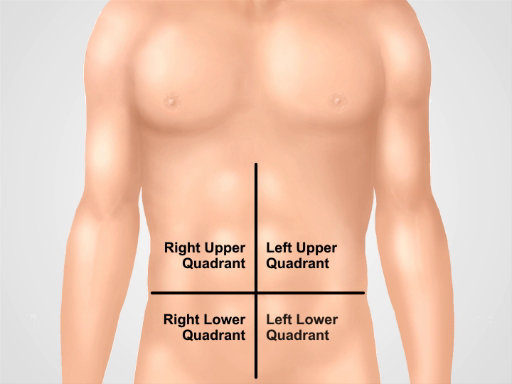
Figura 1. Cuatro cuadrantes abdominales. El abdomen se puede dividir en cuatro regiones por dos líneas imaginarias que se intersecan en el ombligo: cuadrante superior derecho (a menudo señalado como en CSD), cuadrante superior (LUQ), cuadrante inferior derecho (CID) y la izquierda cuadrante inferior (CII) se muestran a la izquierda.
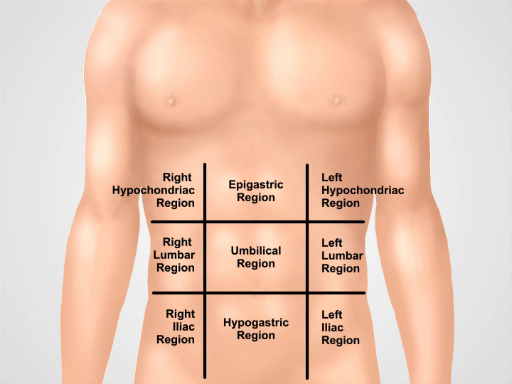
Figura 2. Nueve regiones abdominales. Midclavicular líneas y planos subcostal y intertubercular separan el abdomen en nueve regiones: región epigástrica, región derecha hipocondríaco, región izquierda hypochondriac, región umbilical, región lumbar derecha, región lumbar izquierda, hypogastric de la región, región inguinal derecha y región inguinal izquierda. Términos para epigástrica y umbilical hipogástrica y regiones suprapúbica son los más utilizadas en la práctica clínica.
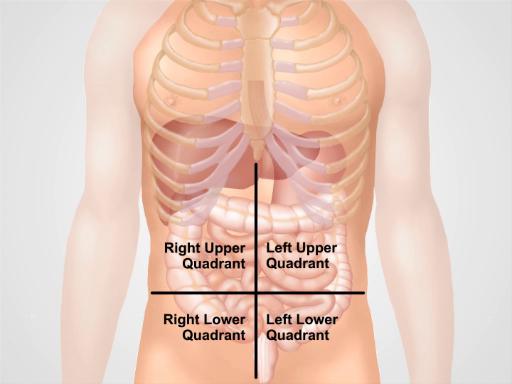
Figura 3. Ubicación de los diferentes órganos en las cuatro regiones abdominales. Órganos en la cavidad abdominal y su ubicación con respecto a los cuatro cuadrantes abdominales.