The rabbit blood shunt model of SAH described in this report produces EBI in the hippocampus (Figure 2A, B), basal cortex (Figure 2A, B), and cerebral vasculature (Figure 2C) as early as 24 hr after injury and shows a characteristic blood distribution (Figure 2D)8. In addition, the model triggers moderate to severe degrees of DCVS on day three after SAH induction (Figure 3)10. The mortality rate is 20 – 30% due to respiratory arrest or severe bradycardia at the time of acute SAH. Almost all rabbits show progressive aggravation of neurological deficits from days 1 – 310. At that time point the animals are under complete anesthesia. From a technical point of view, the blood shunt model allows for both examiner-independent and controllable SAH induction (Figure 4).

Figure 1. Outer skull landmarks for CBF and ICP probes. (Reproduced with permission from the Journal of Neuroscience Methods 201:322 – 326) 9 Schematic drawing depicts the placement of intraparenchymal CBF and ICP probes in the frontal lobes and in the right olfactory bulb. CBF probes are placed 4 – 5 mm anterior and parasagittal to the bregma. ICP probes are placed in the midpupillary line in caudal–rostral direction at a distance of 1 – 2 mm from midsagittal line. Intraparenchymal CBF (Panels A and B) and ICP (Panels C and D) probes are shown in sagittal and coronal planes of T2-weighted MRIs. Note their relation to the ventricles. CBFl = left frontal burrhole for cerebral blood flow probes. CBFr = right frontal burr hole for cerebral blood flow probes. ICP = position of burr hole for intracranial pressure probes. *Bregma; **lambda. Please click here to view a larger version of this figure.
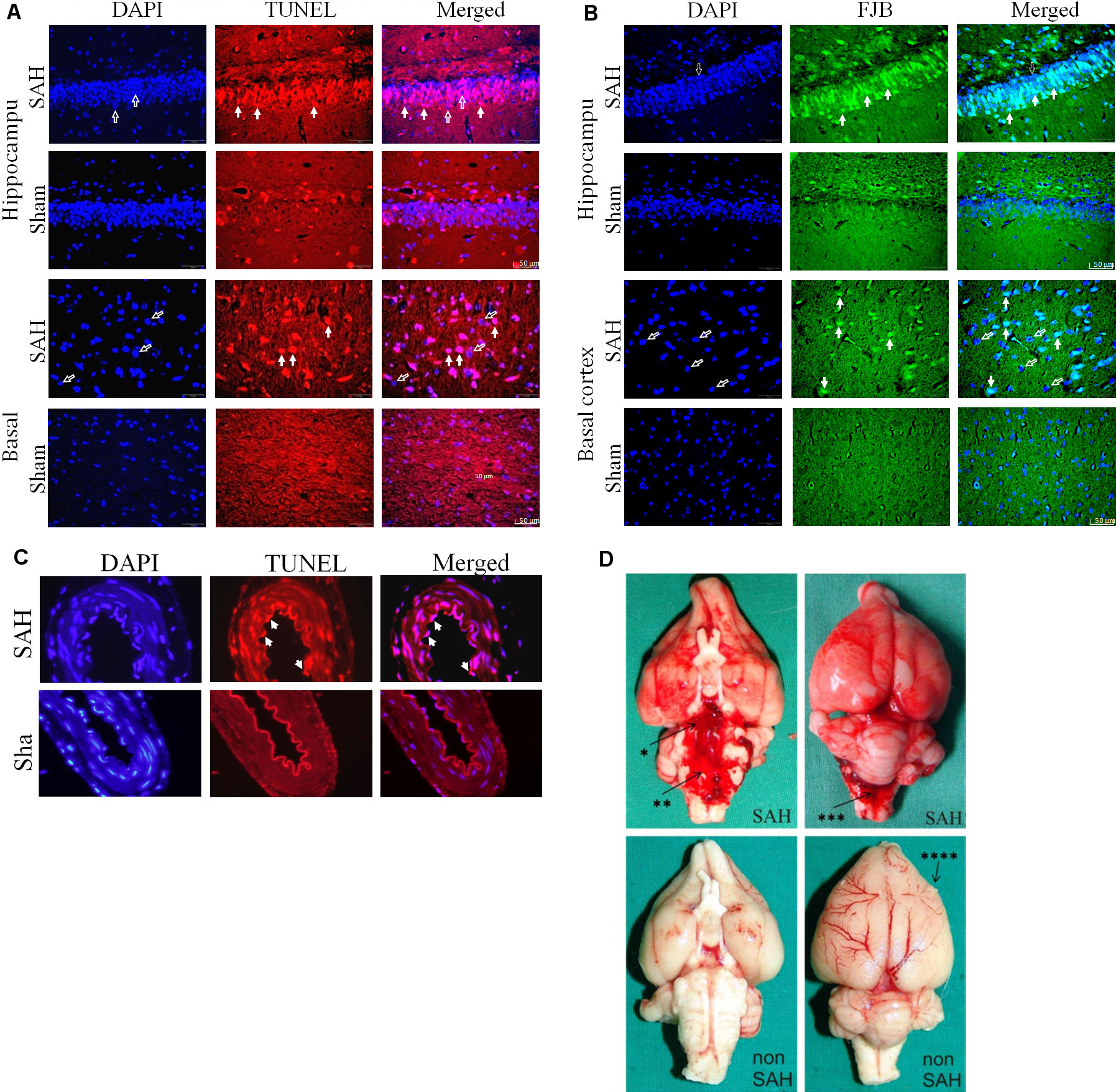
Figure 2. Early brain injury after subarachnoid hemorrhage. (Reproduced with permission from the Journal of Neuroscience Methods 208, 138 – 145 8 and the Journal of Neuroscience Methods 191:227 – 233) 10. TUNEL staining showed apoptosis in the hippocampus (A) and basal cortex (B) of SAH animals. Neurodegeneration was analyzed by FJB (Fluoro-jade stain) positive cells colocalized with DAPI. Colocalization with DAPI (left column) revealed that TUNEL positive staining (middle column) was localized in the nucleus (right column). Open arrows show DAPI positive nuclear staining. Solid arrows indicate TUNEL positive or FJB-positive cells. Scale bar = 50 μm. (C) Apoptosis and neurodegeneration are depicted 24 hr post SAH in basilar artery endothelial cells. Filled arrows indicate TUNEL- positive apoptotic, swollen, and detached endothelial cells. Scale bar = 50 μm. (D) Gross examination of the brain shows extended blood distribution on the ventral and dorsal surface of the brain and basal cisterns 24 hr after SAH induction as compared to sham-operated animals. * = basal cistern; ** = prepontine cistern; *** = cisterna magna; right frontal cortex lesion from the perioperative ICP monitor tip (**** = ICP probe lesion). Please click here to view a larger version of this figure.
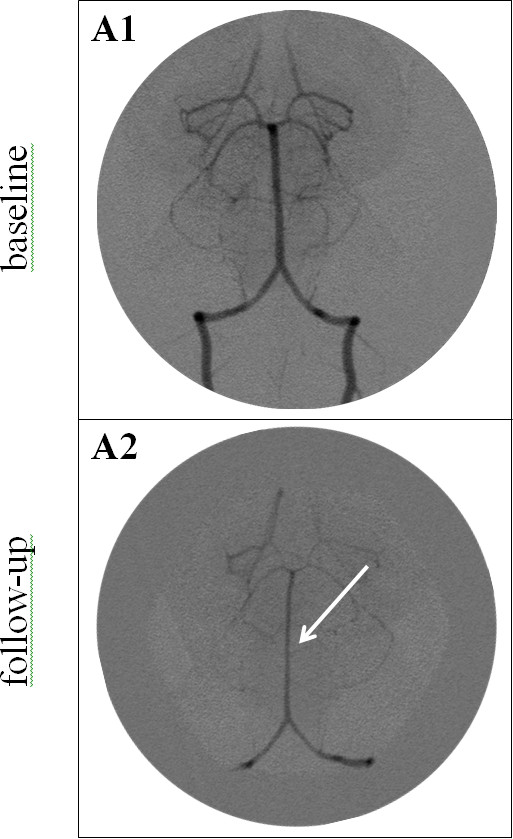
Figure 3. Vertebrobasilar angiograms before (A1) and after (A2) SAH induction. Baseline angiogram (A1) shows normal vessel diameter of the vertebral and basilar arteries. Three days after SAH induction (A2), angiogram shows a diffuse narrowing of the basilar (arrow) and vertebral arteries. Please click here to view a larger version of this figure.

Figure 4. ICP-controlled induction of various degrees of SAH. A key element of the rabbit blood shunt model is the ability to control for various degrees of SAH severity, including the amount of bleeding, an increase in intracranial pressure (ICP), or a reduction in cerebral perfusion pressure (CPP). Figure 4 illustrates the time course of the ICP following the induction of SAH (arrow = opening of the shunt). The curve progression depends on the physiology of the rabbit, primarily the pressure gradient between ICP and mean arterial blood pressure. If ICP reaches a value close to the diastolic blood pressure, the flow in the shunt stops. At that time point either ICP starts to decrease or the ICP value remains on a plateau. If the plateau stays longer than 10 sec the shunt is closed. Controlled SAH can be performed at any ICP level through closure of the shunt before spontaneous thrombosis (X = closure of the shunt). Please click here to view a larger version of this figure.
