These protocols follow the guidelines of our institution's human research ethics committee.
1. Conventional Corneal Collagen CXL (C-CXL)
1. Preparation of the Patient
- 5 days before the surgery, put 1% pilocarpine drops twice a day in the treated eye.
- In the operating room, in aseptic conditions, lie the patient on his/her back.
- Administer topical anesthesia such as oxybuprocaine 0.4%.
- Clean the eye and the skin around the eye with iodine antiseptic twice.
- Use a lid speculum to keep the eye open.
2. Epithelial Removal
- Mark the central 9.0 mm of the cornea with a circle corneal marker.
- Remove the central 7.0 to 9.0 mm of corneal epithelium by mechanical debridement using a blunt spatula.
3. Riboflavin Application
- Apply 0.1% riboflavin with 20% Dextran on the cornea every min for 20 min.
4. UVA Irradiation
- Irradiate the cornea with a 370 nm wavelength UVA light at an irradiance of 3 mW/cm2 (5.4 J/cm2 surface dose) and at a 5 cm working distance for 30 min.

Figure 1: UVA irradiation in C-CXL. The cornea is irradiated with a 370 nm wavelength UVA light at an irradiance of 3 mW/cm2 (5.4 J/cm2 surface dose) and at a 5 cm working distance for 30 minutes. Please click here to view a larger version of this figure.
- During irradiation, apply drops of riboflavin to the cornea every 5 min.
- During irradiation, add topical anesthesia (oxybuprocaine 0.4%) if necessary.
5. End of the Surgery
- Put antibiotic drops (tobramycin 0.3%) and artificial tears (hyaluronate drops 0.18%) into the operated eye.
- Place a soft bandage contact lens at the end of surgery until re-epithelialization is complete. Re-epithelialization usually takes 3 days.
- Prescribe analgesics such as paracetamol (500 mg) plus codeine (30 mg), 6 pills a day.
- After corneal re-epithelialization, initiate topical therapy with steroids (topical dexamethasone 1 mg/ml) and continue for 3-4 weeks. Plus, use artificial tears 4 times a day for 1 month.
2. Accelerated Corneal Collagen CXL (A-CXL)
1. Preparation of the Patient
- 5 days before the surgery, put 1% pilocarpine drops twice a day in the treated eye.
- In the operating room, in aseptic conditions, lie the patient on his/her back.
- Administer topical anesthesia such as oxybuprocaine 0.4%.
- Clean the eye and the skin around the eye with iodine antiseptic twice.
- Use a lid speculum to keep the eye open.
2. Epithelial Removal
- Mark the central 9.0 mm of the cornea with a circle corneal marker
- Remove the central 7.0 to 9.0 mm of corneal epithelium by mechanical debridement using a blunt spatula.
3. Riboflavin Application
- Apply 0.1% riboflavin without Dextran on the cornea every 2 min for 10 min.
4. UVA Irradiation
- Irradiate the cornea with a 370 nm wavelength UVA light at an irradiance of 30 mW/cm2 (5.4 J/cm2 surface dose) and at a 5 cm working distance for 3 min.
- During the irradiation, add topical anesthesia (oxybuprocaïne 0.4%) if necessary.
5. End of the Surgery
- Place antibiotic drops (tobramycin 0.3%) and artificial tears (hyaluronate drops 0.18%) into the operated eye.
- Place a soft bandage contact lens at the end of surgery until re-epithelialization is complete. Re-epithelialization usually takes 3 days.
- Prescribe analgesics such as paracetamol (500 mg) plus codeine (30 mg), 6 pills a day.
- After corneal re-epithelialization, initiate topical therapy with steroids (topical dexamethasone 1 mg/ml) and continue for 3-4 weeks. Plus, use artificial tears 4 times a day for 1 month.
3. Iontophoresis (I-CXL)
1. Preparation of the Patient
- 5 days before the surgery, put 1% pilocarpine drops twice a day in the treated eye.
- In the operating room, in aseptic conditions, lie the patient on his/her back.
- Administer topical anesthesia such as oxybuprocaine 0.4%.
- Clean the eye and the skin around the eye with iodine antiseptic twice.
- Use a lid speculum to keep the eye open.
2. Position the Iontophoresis Device.
- Apply the sticky passive electrode on the forehead under the operative field.
- Apply the active electrode, a suction ring, to the open eye. Center the suction ring on the periphery of the cornea before releasing the suction.

Figure 2. Iontophoresis device. The passive electrode is applied on the forehead under the operative field and the active electrode, a suction ring, is applied to the open eye. Please click here to view a larger version of this figure.
3. Riboflavin Application
- Fill the suction ring with hypoosmolar 0.1% riboflavin without Dextran.

Figure 3. Riboflavin application in I-CXL. The suction ring is filled with hypoosmolar 0.1% riboflavine without Dextran. Please click here to view a larger version of this figure.
- Start the electrical current at 0.2 mA and gradually increase to 1.0 mA for a total iontophoresis time of 5 min (Figure 4).

Figure 4. Iontophoresis device for riboflavin penetration. The electrical current is initially 0.2 mA and gradually increased to 1.0 mA. Total iontophoresis time is 5 minutes. Please click here to view a larger version of this figure.
4. UVA Irradiation
- Irradiate the cornea with a 370 nm wavelength UVA light at an irradiance of 10 mW/cm2 (5.4 J/cm2 surface dose) and at a 5 cm working distance for 9 min.
- During the irradiation, add topical anesthesia (oxybuprocaïne 0.4%) if necessary.
5. End of the Surgery
- Place antibiotic drops (tobramycin 0.3%) and artificial tears (hyaluronate drops 0.18%) into the operated eye.
- Prescribe analgesics such as paracetamol (500 mg) plus codeine (30 mg), 6 pills a day.
- After surgery, initiate topical therapy with steroids (topical dexamethasone 1mg/ml) and continue for 3-4 weeks. Plus, use artificial tears 4 times a day for 1 month.
The corneal demarcation line was visible in AS OCT in 92% of cases at a mean depth of 301.6 µm (SD, 73.6)
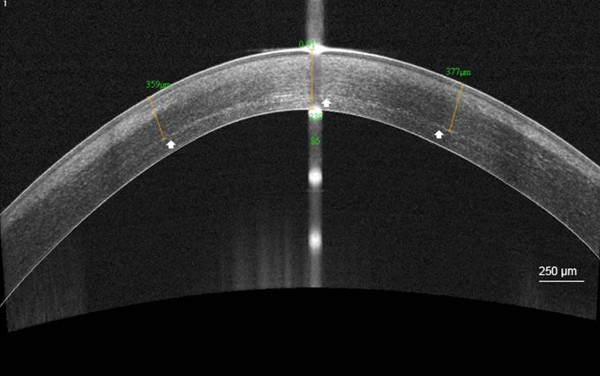
Figure 5. Demarcation line after C-CXL. High-resolution corneal anterior segment optical coherence tomography scan (AS OCT) visualizing the corneal stromal demarcation line at a mean depth of 358 µm (white arrow), 1 month after conventional corneal collagen cross-linking (C-CXL). Scale bar 250 µm. Please click here to view a larger version of this figure.
1 month after C-CXL, whereas after A-CXL it was seen in 85.5% of cases at a mean depth of 183.1 µm (SD, 39.6).

Figure 6. Demarcation line after A-CXL. High-resolution corneal anterior segment optical coherence tomography scan (AS OCT) visualizing the corneal stromal demarcation line at a mean depth of 176 µm (white arrow), 1 month after accelerated corneal collagen cross-linking (A-CXL). Scale bar: 250 µm. Please click here to view a larger version of this figure.
Finally, after I-CXL, the corneal demarcation line was only seen in 46.5% of cases at a mean depth of 214 µm (SD, 37.5). The differences in corneal demarcation line depth following either C-CXL, A-CXL or I-CXL were statistically significant (p <0.001 and p = 0.01). The demarcation line was present significantly more often after C-CXL and A-CXL than after I-CXL (p = 0.005).

Figure 7. Demarcation line after I-CXL. High-resolution corneal anterior segment optical coherence tomography scan (AS OCT) visualizing the corneal stromal demarcation line at a mean depth of 238.5 µm (white arrow), 1 month after iontophoresis (I-CXL). Scale bar: 250 µm. Please click here to view a larger version of this figure.
No intra or postoperative complications were detected in patient follow-ups within 6 months after application of any of the three protocols, including no significant differences in endothelial cell counting. Moreover, the maximum K-value (Kmax) remained stable for each of the protocols after a 6 month follow-up.

Table 1. Efficacy and safety of each protocol of CXL. Evolution of the maximum K-value (dioptry, D) and the endothelial density following conventional (C-CXL), accelerated (A-CXL), and iontophoresis (I-CXL) cross-linking.
For each of the protocols, in the 1-3 month postoperative period, anterior stromal edema with extracellular lacunae and fragmented keratocyte nuclei was observed with IVCM. At 6 months, repopulation of the anterior stroma with keratocyte nuclei was seen and was greater after I-CXL than after the two other protocols. The demarcation between cross-linked and non-cross-linked corneal stroma was seen as a region where keratocytes became elongated and surrounded by large hyper-reflective stromal bands.

Figure 8.: Microstructural corneal changes after C-CXL. In vivo confocal microscopy scans (IVCM) of the corneal stroma obtained 1 month after conventional collagen cross-linking (C-CXL): anterior stromal edema with hyper-reflective cytoplasm (white arrows) and extracellular lacunae (asterisks) are observed. Scale bar: 50 µm.
