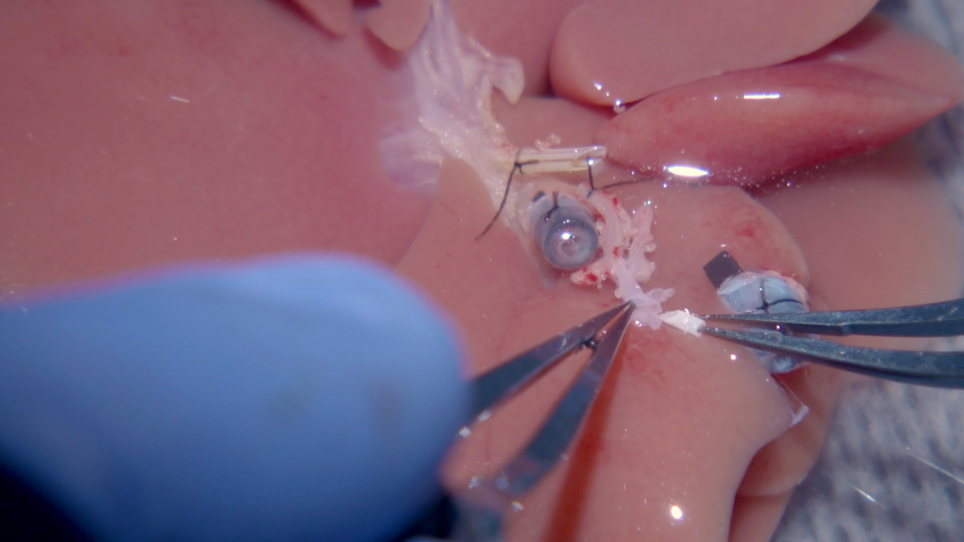
Suprahepatic vena kava (SHVC) yeniden inşası sıçan orthotopic karaciğer nakli zor bir adım kalır. Bu makalede, bir roman manyetik anastomoz tekniği kullanarak Sıçanlarda SHVC yeniden inşası için adım adım bir protokol gösteriyoruz.