The described operative techniques create a novel animal model of a chronic aortic hypoxia-induced aneurysm by using a combination of polyurethane catheter insertion and suture ligation of the infrarenal abdominal aorta in rats. The rats described in the Protocol section were euthanized 28 days after the procedure. The aortas were harvested and imaged to visualize aneurysm formation. Figure 2 shows development of the fusiform AAA. The upper and lower ends of the aorta in ex vivo have a normal diameter without dilatation. Aortic diameters were measured using transabdominal ultrasonography (Figure 3). The diameter generally reaches its maximum size at about 14 days after the procedure; thereafter, it remains unchanged or slightly increases. Figure 4 shows the histopathological image of the aneurysm at its maximum diameter after EVG staining. The image of the tissue on day 28 (aneurysm) showed prominent degradation of elastic fibers compared to that on day 0.

Figure 1: Surgical procedures to induce an abdominal aortic aneurysm (AAA).
(A) The infrarenal aorta is exfoliated from the surrounding tissue. (B) A polyurethane catheter cut 10 mm long is inserted through a small incision in the aorta. (C) The incision is repaired with an 8-0 monofilament suture and blood flow is restored. (D) The aorta is ligated with a 5-0 silk suture over the inserted catheter. Scale bar = 5 mm. Please click here to view a larger version of this figure.
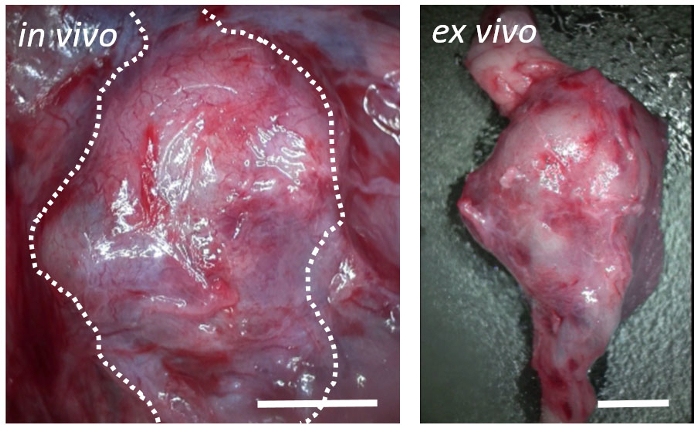
Figure 2: Postoperative representative results.
Macroscopic view on postoperative day 28 showing development of fusiform abdominal aortic aneurysms. The elevated margin of the retroperitoneum corresponds to the outer edge of the aneurysm (broken lines; left). The upper and lower ends of the aorta in ex vivo are normal (right). Scale bar = 3 mm. Please click here to view a larger version of this figure.
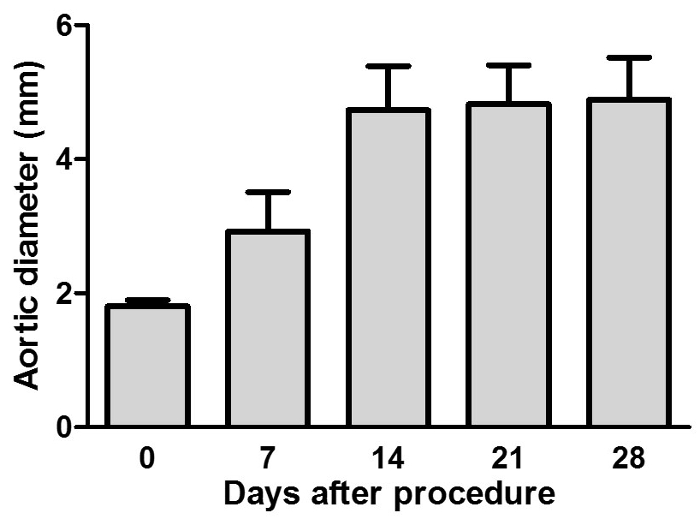
Figure 3: Maximum aortic diameters measured using transabdominal ultrasonography.
The aortic diameter steadily increased in this rat model. Aortic diameters are presented as a mean ± standard deviation (n = 12). Please click here to view a larger version of this figure.
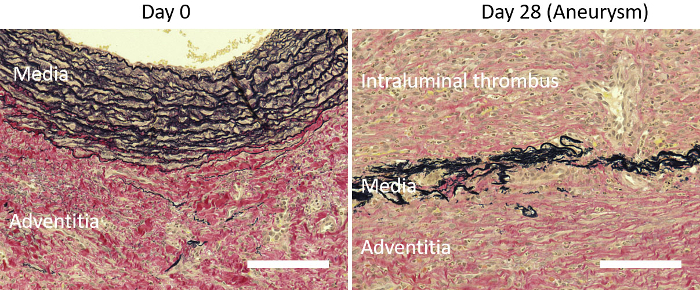
Figure 4: Representative images of aneurysmal tissue with Elastica van Gieson staining.
Histological evaluation with EVG staining showing the degenerative elastic lamina in the media and formation of an intraluminal thrombus 28 days after the procedure (right). Elastic fiber fragmentation in the aortic media and sparse collagen fiber in the aortic adventitia are observed on day 28. Day 0 is before the procedure (left). Scale bar = 500 µm. Please click here to view a larger version of this figure.
