A total of 40 patients with BPH who underwent DiLEP were included in one of our studies. An independent sample t-test was used as the statistical method. All patients successfully completed the operation. Almost all of the patients had the catheter removed within 5 days postoperative (Table 1). All patients returned to the hospital for follow-up examinations in the 1st, 3rd, and 12th months postoperatively. The International Prostate Symptom Score (IPSS)11 and Quality of Life (QoL)1 tools were used to screen for, rapidly diagnose, track the symptoms of, and guide the management of BPH. These can also be used to evaluate the efficacy of the BPH treatment. Compared to the baseline values, the International Prostate Symptom Score (IPSS) significantly decreased to 38.15%, 31.92%, and 18.70% at 1, 3, and 12 months postoperatively, respectively (all p < 0.001), and the QoL significantly decreased to 57.89%, 43.94%, and 20.78% (all p < 0.001, respectively). For objective parameters, compared to the baseline, the mean Qmax increased nearly 3x, and the mean postvoid residual during follow-up decreased nearly 4x. Compared to the preoperative values, postoperatively, the prostate volume decreased dramatically (p < 0.001) (Table 2).
The peri- and postoperative complications reported during this study are presented in Table 3. According to the modified Clavien Dindo classification system12, a widely used and authoritative tool for grading surgical complications, no intraoperative patient had complications, and only four cases reported Grade 1 postoperative complications12.

Figure 1: Circularly incise the bladder neck mucosa with a laser. Please click here to view a larger version of this figure.

Figure 2: Circularly incise the prostatic urethra mucosa at the proximal end of verumontanum with a laser. Please click here to view a larger version of this figure.

Figure 3: Incise the left lobe and right lobe at the apex of the prostate at 12 o'clock. Please click here to view a larger version of this figure.

Figure 4: Circularly incise the bladder neck mucosa with a laser. Please click here to view a larger version of this figure.

Figure 5: Find the surgical capsule at the 5 and 7 o'clock positions of the apex of the prostate and connect the 5 and 7 o'clock surgical capsule positions with a laser. Please click here to view a larger version of this figure.

Figure 6: In a counterclockwise direction, enucleate the right lobe at the 6 and 12 o'clock positions from the apex of the prostate to the bladder neck. Please click here to view a larger version of this figure.

Figure 7: In a clockwise direction, enucleate the left lobe at the 6 and 12 o'clock positions from the apex of the prostate to the bladder neck. Please click here to view a larger version of this figure.
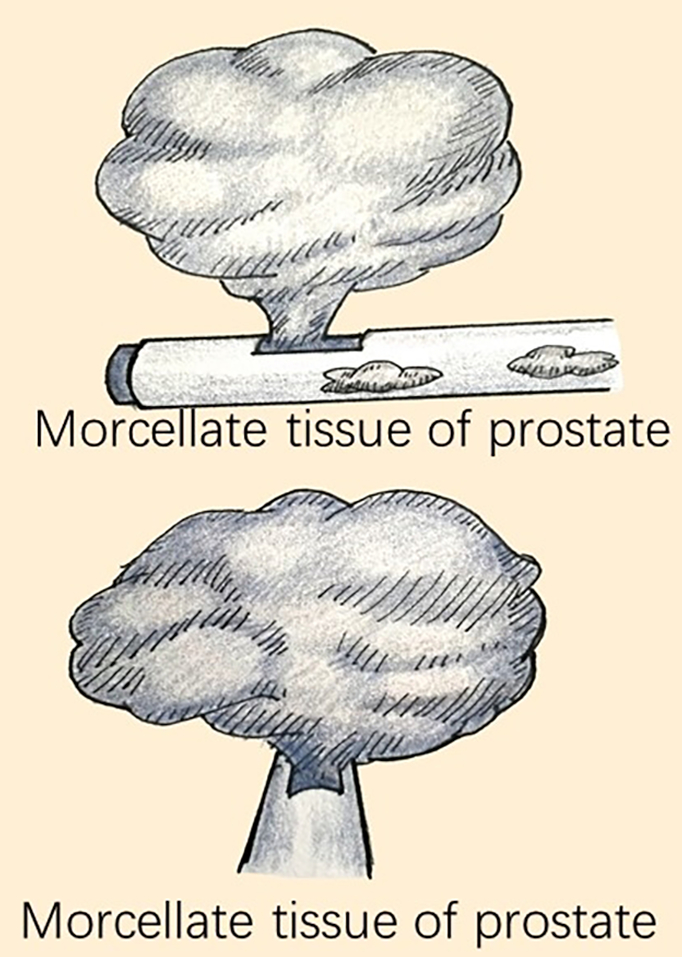
Figure 8: Cut the enucleated prostatic tissue into small pieces using a morcellator and then remove the tissues from the bladder. Please click here to view a larger version of this figure.
| Parameters | Data |
| Age (y) | 73.35±7.84 |
| Prostate volume (ml) | 106.40±19.01 |
| Operative time (min) | 71.18±16.55 |
| Perfusion fluid volume (L) | 28.02±13.80 |
| Postoperative irrigation time (h) | 13.47±1.83 |
| Decrease in hemoglobin (g/L) | 2.62±1.24 |
| Catheter duration (d) | 4.25±0.08 |
| Hospital stay (d) | 4.60±0.77 |
| Follow-up time(m) | 12.45±1.75 |
| Data are shown as mean ± SD;BPH: Benign prostatic hyperplasia; diode laser enucleation of the prostate; SD: Standard deviation | |
Table 1: Perioperative data of 40 patients with BPH who underwent DiLEP.
| Parameters | Pre-operative | 1m | 3m | 12m | P-value |
| Qmax (ml/min) | 7.12±2.94 α,β,γ | 21.19±2.18 | 22.24±2.02 | 19.73±1.80 | <0.001 |
| PVR(ml) | 113.22±33.56 α,β,γ | 27.30±3.98 | 25.05±4.21 | 31.10±6.65 | <0.001 |
| IPSS | 23.15±7.44 α,β,γ | 8.37±2.49 | 7.37±1.94 | 4.33±1.79 | <0.001 |
| QOL | 3.80±0.88 α,β,γ | 2.20±0.89 | 1.67±0.65 | 0.79±0.66 | <0.001 |
| PV(ml) | 106.40±19.01 | —— | —— | 22.08±4.28 | <0.001 |
| Qmax = maximum flow rate; PVR = postvoid residual; IPSS = International Prostate Symptom Score; QoL = quality of life; PV = prostate volume | |||||
| α:Significant differences between pre- and post-operative 1 month groups; β:Significant differences between pre- and post-operative 3 months groups; γ:Significant differences between pre- and post-operative 12 month |
|||||
Table 2: Data at baseline and at 1, 3, and 12 months postoperatively parameters.
| Complications | Patients, n (%) | Grade |
| Intraoperative | ||
| Prostate capsule perforation | 0 | 3b |
| Blood transfusion | 0 | 2 |
| TURP syndrome | 0 | 4 |
| Bladder wall injury | 0 | 2 |
| Ureteric orifce injury | 0 | 2 |
| Urethra sphincter injury | 0 | 2 |
| Postoperative | ||
| Bladder convulsion | 2 (5%) | 1 |
| Urge urinary incontinence | 2 (5%) | 1 |
| Stress urinary incontinence | 0 | 2 |
| Re-place the catheter | 0 | 1 |
| Complications were graded according to the modifed Clavien-Dindo classifcation system | ||
Table 3: Peri- and post-operative complications of 40 patients with BPH who underwent DiLEP.
