腹部考试 II: 打击乐
English
Share
Overview
资料来源: 亚历山大 · 戈德法布,MD,助理医学教授,贝斯以色列女执事医疗中心,马
医疗打击乐基于音调诱发体壁敲打的声音之间的不同。对攻丝的听觉反应取决于的轻松体壁震动,并受到潜在的器官,中风和体壁的状态的强度。有三个主要医疗敲击声音: 共振 (肺听到)、 鼓音 (在充满空气的肠管听到) 和迟钝 (听说流体或固体器官)。浊音与鼓音或共振对比允许尺寸的确定和边距的机关和群众,以及积液的鉴别和整合领域。打击乐仍然错综复杂的物理诊断一部分因为它首先介绍了 200 多年前,和在考试的肺部和腹部中尤其有用。
腹部检查的一部分,打击乐如下目测和听诊。考官应首先叩每年的 9 个腹部区域 (腹壁下区、 右胁,左胁区域、 脐区、 腰椎右侧区域、 左的腰部、 下腹、 右腹股沟和左腹股沟区)。诱发打击乐的温柔是不正常的和应怀疑腹膜的炎症。如充气肠管位于腹壁最接近,打击乐在腹腔内的大部分地区引起主要鼓膜的声音。大面积的浊音的存在应该提示脏器肿大、 腹内肿块或流体的评定。
除了评估腹部气的分布与数量,腹部的考试应由打击乐包括肝脏和脾脏大小的估计。由于肝和脾都附有肋骨笼,考官应叩在低前胸。通常情况下,一个希望听到沉闷的声音,右前胸在肝脏,敲击乐器和打击乐的左前胸在胃的气泡和 (图 1) 结肠脾曲鼓室声。
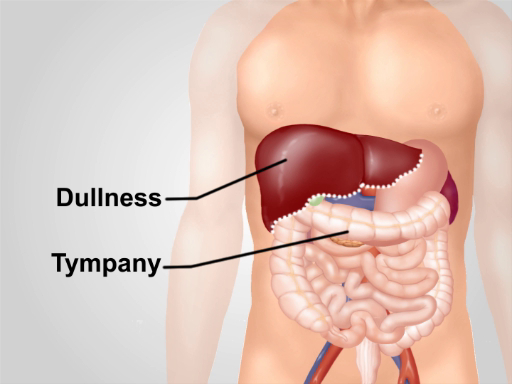
图 1。正常的打击乐的笔记在腹部。除了面积超过肝脏的右下胸迟钝,鼓音是听到在该地区的主导声音。
Procedure
Applications and Summary
Despite rapid advances in imaging techniques, abdominal percussion remains an essential part of a physical examination. Correct percussion technique is critical for this method to be effective. The percussion strike should be kept the same over the entire abdomen. All the information obtained during the patient’s interview and full physical examination, and a good knowledge of differential diagnoses of each pathological sign is essential for proper interpretation of any findings. For example, a false increase of liver span on percussion can result from right lung consolidation and/or a pleural effusion. One should also be aware of the limitation of the method and the sensitivity of each diagnostic maneuver. While percussion is only moderately accurate in detecting hepato-and splenomegaly, abnormal findings should prompt further clinical evaluation.
Transcript
Percussion is a critical part of the abdominal examination; therefore, learning the correct technique is essential for any physician aiming to make quick, yet accurate diagnosis of gastrointestinal pathologies. As you might know, medical percussion is based on the difference in pitch between the sounds elicited by tapping on the body wall. The sounds produced during abdominal percussion can help detect pathologies like organomegaly, intra-abdominal masses, and fluid accumulation. This video will illustrate the major anatomical areas to be percussed during an abdominal exam, and the steps and findings of this procedure.
First, let’s talk about the expected abdominal percussion sounds and their interpretations. As the air-filled bowel loops are positioned in the closest proximity to the abdominal wall, percussion over most parts of the abdominal cavity elicits a predominantly tympanic sound… Notice that this sound is relatively long, high pitched, and loud.
Percussion over dense organ tissues, like the spleen or the liver, produces a dull sound… Therefore, the contrast between dullness versus tympany allows for determination of the margins of these organs and thus help in detection of conditions like hepatomegaly or splenomegaly. Dull sounds are also produced on percussing areas filled with fluid and feces. Therefore, by percussing one can predict the cause of protuberant abdomen, which helps in diagnosis of conditions like ascites.
With this background in mind, let’s review a detailed step-wise procedure for abdominal percussion. Explain the procedure to the patient and obtain their consent before starting with the exam. Drape the patient appropriately to expose the torso area and perform light percussion over each of the nine abdominal regions.
Listen to the intensity, pitch, and duration of the percussion note. Normally, tympanic sound produced by air in the bowel loops will be heard… As you percuss, watch the patient’s face for any signs of discomfort. Ask the patient if they are experiencing any tenderness. Tenderness on percussion is abnormal and can indicate peritoneal inflammation.
After abdominal area, percuss the lower anterior chest, above the costal margins. Dull sound on the right, over the liver is expected… On the left, one should hear tympany over the gastric air bubble and the splenic flexure of the colon… Following that, move to the area of pubic symphysis. Again, this should yield a tympanic sound…dullness indicates enlarged uterus or distended bladder.
Next step is to determine the liver span. Start by locating the right midclavicular line. Starting in the area of tympany below the umbilicus, lightly percuss in the right midclavicular line moving upwards… Make a mark where the tympany changes to dullness with a skin pencil. This is the lower border of the liver. Then, starting at the nipple line, again percuss in the right midclavicular line moving downwards. Note the point where the resonant sound changes to dullness…and mark it with a skin pencil. This is the upper border of the liver. Measure the distance between upper and lower border in centimeters. The liver span is normally 6-12 cm.
Following the liver span measurement, percuss to detect splenomegaly. The two maneuvers for this include Percussion of the Traube’s space and the Castell’s method. For percussion of the Traube’s space, make sure that the patient’s left arm is slightly abducted, and percuss from the medial to lateral border of this area. Overall dullness on percussion, or reduction of the area of tympany can indicate spleen enlargement. For the Castell’s method, percuss in the anterior axillary line in the lower intercostal space. Ask the patient to take a deep breath and percuss again. Normally, the percussion tone is tympanic on both inspiration and expiration. If the percussion note is dull, or becomes dull on inspiration, splenomegaly should be suspected.
Lastly, percussion is helpful to detect the cause of a protuberant abdomen. If the patient has a protuberant abdomen, percuss from the umbilicus in a lateral direction and with the skin pencil make a mark of the point where the tympanic sound changes to dullness. Then, ask the patient to roll on their side and repeat the percussion starting from the top and make a second mark when the tympanic sound changes to dull. If abdominal fluid were present, the level of dullness on the side would shift upwards toward the umbilicus, compared to the level of dullness in supine position.
You’ve just watched JoVE’s video on percussion to be performed during an abdominal exam. You should now know the important abdominal percussion steps and understand differential diagnoses that can be performed by proper interpretation of percussion findings. As always, thanks for watching!