Fonte: Alexander Goldfarb, MD, Assistente Professore di Medicina, Beth Israel Deaconess Medical Center, MA
La percussione medica si basa sulla differenza di tono tra i suoni suscitati toccando la parete del corpo. La risposta uditiva al tapping dipende dalla facilità con cui vibra la parete del corpo ed è influenzata dagli organi sottostanti, dalla forza del colpo e dallo stato della parete corporea. Ci sono tre principali suoni di percussioni mediche: risonanza (ascoltata sui polmoni), timonica (ascoltata sopra i loop intestinali pieni d’aria) e ottusità (ascoltata su organi fluidi o solidi). Il contrasto tra ottusità e timosanica o risonanza consente di determinare le dimensioni e i margini di organi e masse, nonché di identificare l’accumulo di liquidi e le aree di consolidamento. La percussione rimane una parte intricata della diagnosi fisica da quando è stata introdotta per la prima volta più di 200 anni fa ed è particolarmente utile nell’esame dei polmoni e dell’addome.
Come parte di un esame addominale, la percussione segue l’ispezione visiva e l’auscultazione. L’esaminatore dovrebbe prima percuss su ciascuna delle nove regioni addominali (regione epigastrica, regione ipocondriaca destra, regione ipocondriaca sinistra, regione ombelicale, regione lombare destra, regione lombare sinistra, regione ipogastrica, regione inguinale destra e regione inguinale sinistra). La tenerezza suscitata dalle percussioni è anormale e si dovrebbe sospettare un’infiammazione peritoneale. Poiché le anse intestinali piene d’aria sono posizionate nelle immediate vicinanze della parete addominale, la percussione sulla maggior parte delle parti della cavità addominale suscita un suono prevalentemente timpanico. La presenza di ampie aree di ottusità dovrebbe richiedere una valutazione per organomegalia, masse intra-addominali o fluidi.
Oltre a valutare la quantità e la distribuzione del gas addominale, un esame addominale dovrebbe includere una stima delle dimensioni del fegato e della milza mediante percussione. Poiché il fegato e la milza sono coperti dalla gabbia toracica, l’esaminatore dovrebbe percussore anche sul torace anteriore inferiore. Normalmente, ci si aspetta di sentire un suono sordo sulle percussioni del torace anteriore destro sul fegato e un suono timpanico sulla percussione del torace anteriore sinistro sulla bolla d’aria gastrica e sulla flessione splenica del colon (Figura 1).
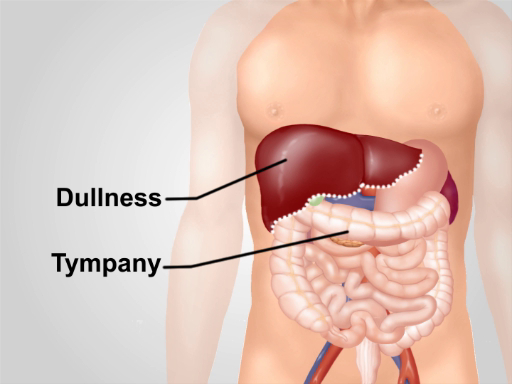
Figura 1. Normali note di percussione sulla regione addominale. Con l’eccezione di un’area di ottusità sul fegato nel torace anteriore inferiore destro, il timpano è il suono predominante sentito sulla regione.