Fuente: Alexander Goldfarb, MD, profesor de medicina, centro médico Beth Israel Deaconess, MA
Percusión médica se basa en la diferencia de tono entre los sonidos sacados por los golpecitos en la pared del cuerpo. La respuesta auditiva a tocar depende de la facilidad con que vibra la pared del cuerpo y está influenciada por los órganos subyacentes, fuerza de la carrera y el estado de la pared del cuerpo. Hay tres sonidos de percusión médica principal: resonancia (escuchado en los pulmones), tympany (oído sobre las asas intestinales llenas de aire) y matidez (oído sobre órganos sólidos o líquidos). El contraste entre la tardanza vs tympany o resonancia permite la determinación del tamaño y márgenes de órganos y masas, así como la identificación de la acumulación de líquido y áreas de consolidación. Percusión es una parte intrincada de la diagnosis física ya que fue introducido hace más de 200 años y es especialmente útil en el examen de los pulmones y el abdomen.
Como parte de un examen abdominal, percusión sigue auscultación e inspección visual. El examinador debe percuss primero sobre cada una de las nueve regiones abdominales (región epigástrica, región derecha hipocondríaco, región izquierda hypochondriac, región umbilical, región lumbar derecha, región lumbar izquierda, hypogastric de la región, región inguinal derecha y región inguinal izquierda). Ternura provocada por percusión es anormal, y se debe sospechar inflamación peritoneal. Como las asas intestinales llenas de aire se colocan en la proximidad más cercana a la pared abdominal, la percusión sobre la mayor parte de la cavidad abdominal produce un sonido timpánico predominante. La presencia de grandes áreas de matidez debe incitar la evaluación de organomegalia, masas intrabdominales o líquido.
Además de evaluar la cantidad y distribución de gas abdominal, un examen abdominal debe incluir una estimación del tamaño del bazo y hígado por percusión. Como el hígado y el bazo están cubiertos por la caja torácica, el examinador debe percuss sobre el pecho anterior inferior también. Normalmente, uno espera escuchar sonido mate a la percusión del tórax anterior derecho sobre el hígado y sonido timpánico a la percusión del pecho izquierdo anterior sobre la burbuja de aire gástrica y el ángulo esplénico del colon (figura 1).
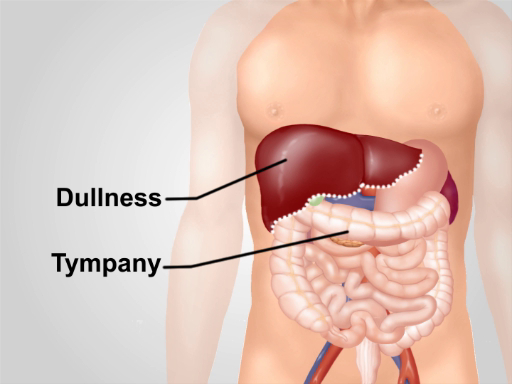
Figura 1. Notas de percusión normal sobre la región abdominal. Con la excepción de un área de matidez sobre el hígado en el tórax anterior inferior derecho, tympany es el sonido predominante oído sobre la región.