Fonte: Alexander Goldfarb, MD, Professor Assistente de Medicina, Beth Israel Deaconess Medical Center, MA
A percussão médica baseia-se na diferença de tom entre os sons provocados por toques na parede do corpo. A resposta auditiva ao toque depende da facilidade com que a parede do corpo vibra, e é influenciada por órgãos subjacentes, força do derrame e o estado da parede do corpo. Existem três sons principais de percussão médica: ressonância (ouvida sobre os pulmões), timpano (ouvido sobre as alças intestinais cheias de ar) e tédio (ouvido sobre fluido ou órgãos sólidos). O contraste entre o embotamento vs. tympany ou ressonância permite a determinação do tamanho e margens de órgãos e massas, bem como a identificação do acúmulo de fluidos e áreas de consolidação. A percussão continua sendo uma parte intrincada do diagnóstico físico desde que foi introduzida pela primeira vez há mais de 200 anos, e é especialmente útil no exame dos pulmões e abdômen.
Como parte de um exame abdominal, a percussão segue inspeção visual e auscultação. O examinador deve primeiro percuss sobre cada uma das nove regiões abdominais (região epigástrica, região hipocondríaca direita, região hipocondríaca esquerda, região umbilical, região lombar direita, região lombar esquerda, região hipogástrica, região inguinal direita e região inguinal esquerda). A ternura provocada pela percussão é anormal, e deve-se suspeitar de inflamação peritoneal. À medida que as alças intestinais cheias de ar são posicionadas na proximidade mais próxima da parede abdominal, a percussão sobre a maioria das partes da cavidade abdominal provoca um som predominantemente tirapônico. A presença de grandes áreas de tédio deve solicitar a avaliação de organomegaly, massas intra-abdominais ou fluidos.
Além de avaliar a quantidade e distribuição de gás abdominal, um exame abdominal deve incluir uma estimativa do tamanho do fígado e do baço por percussão. Como o fígado e o baço estão cobertos pela caixa torácica, o examinador deve percuss sobre o peito anterior inferior também. Normalmente, espera-se ouvir som maçante na percussão do peito anterior direito sobre o fígado, e som timpônico na percussão do peito anterior esquerdo sobre a bolha de ar gástrico e o flexão esplênico do cólon(Figura 1).
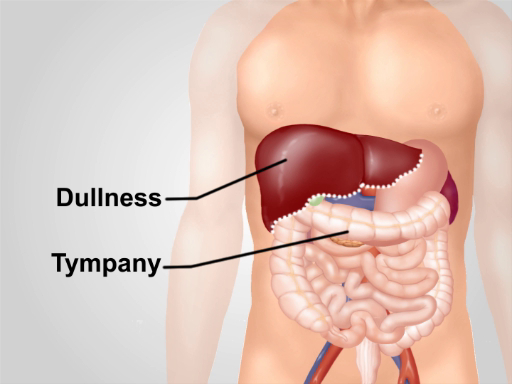
Figura 1. Notas normais de percussão sobre a região abdominal. Com exceção de uma área de tédio sobre o fígado no peito anterior inferior direito, tiranpania é o som predominante ouvido sobre a região.