Source : Alexander Goldfarb, MD, professeur de médecine, Beth Israel Deaconess Medical Center, MA
Percussions médicale sont basée sur la différence de hauteur entre les sons obtenue en tapant sur la paroi du corps. La réponse auditive aux écoutes dépend de la facilité avec laquelle la paroi du corps vibre et est influencée par des organes sous-jacents, force de la course et l’état de la paroi du corps. Il y a trois sons de percussion médical principal : résonance (entendu sur les poumons), tympany (entendu sur les boucles de l’intestin rempli d’air) et l’ennui (entendu sur les organes liquides ou solides). Le contraste entre la matité vs tympany ou résonance permet pour la détermination de la taille et les marges des organes et des masses, ainsi que d’identification de l’accumulation de liquide et de consolidation. Percussion reste une partie indissociable du diagnostic physique puisqu’elle a été introduite il y a plus de 200 ans et est particulièrement utile dans l’examen des poumons et abdomen.
Dans le cadre d’un examen abdominal, percussion suit l’auscultation et inspection visuelle. L’examinateur doit tout d’abord percuss sur chacune des neuf régions abdominales (région épigastrique, région droite hypocondriaque, région hypocondriaque gauche, région ombilicale, région lombaire droite, région lombaire gauche, région hypogastrique, région inguinale droite et gauche région inguinale). Tendresse induite par la percussion est anormale, et l’inflammation péritonéale doit être suspectée. Comme les boucles d’intestin rempli d’air sont placés à proximité le plus proche de la paroi abdominale, la percussion sur la plupart des régions de la cavité abdominale provoque un son tympanique principalement. La présence de vastes étendues de la grisaille devrait inciter l’évaluation viscéromégalie, masses intra-abdominale ou fluide.
En plus d’évaluer la quantité et la distribution de gaz abdominaux, un examen abdominal doit inclure une estimation du foie et de la taille de la rate par percussion. Comme le foie et la rate sont couverts par la cage thoracique, l’examinateur devrait percuss sur la poitrine inférieure antérieure aussi bien. Normalement, on s’attend à entendre un bruit sourd à la percussion du thorax droit antérieur sur le foie et son tympan par percussion de gauche poitrine sur la bulle d’air gastrique et la flexure splénique du côlon (Figure 1).
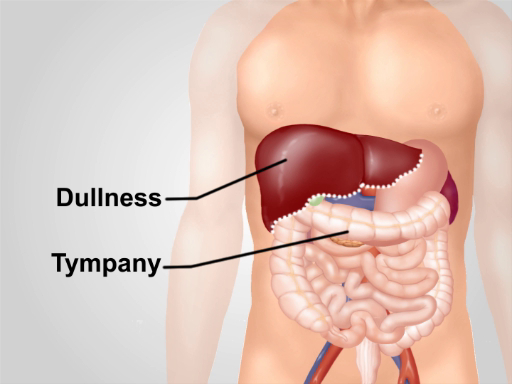
Figure 1. Notes de percussions normale sur la région abdominale. à l’exception d’une superficie de grisaille sur le foie dans la poitrine inférieur droit, tympany est le prédominant son entendu au-dessus de la région.