Percussion is a critical part of the abdominal examination; therefore, learning the correct technique is essential for any physician aiming to make quick, yet accurate diagnosis of gastrointestinal pathologies. As you might know, medical percussion is based on the difference in pitch between the sounds elicited by tapping on the body wall. The sounds produced during abdominal percussion can help detect pathologies like organomegaly, intra-abdominal masses, and fluid accumulation. This video will illustrate the major anatomical areas to be percussed during an abdominal exam, and the steps and findings of this procedure.
First, let’s talk about the expected abdominal percussion sounds and their interpretations. As the air-filled bowel loops are positioned in the closest proximity to the abdominal wall, percussion over most parts of the abdominal cavity elicits a predominantly tympanic sound… Notice that this sound is relatively long, high pitched, and loud.
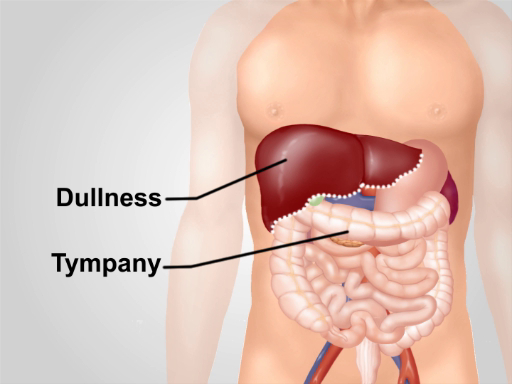
Percussion over dense organ tissues, like the spleen or the liver, produces a dull sound… Therefore, the contrast between dullness versus tympany allows for determination of the margins of these organs and thus help in detection of conditions like hepatomegaly or splenomegaly. Dull sounds are also produced on percussing areas filled with fluid and feces. Therefore, by percussing one can predict the cause of protuberant abdomen, which helps in diagnosis of conditions like ascites.
With this background in mind, let’s review a detailed step-wise procedure for abdominal percussion. Explain the procedure to the patient and obtain their consent before starting with the exam. Drape the patient appropriately to expose the torso area and perform light percussion over each of the nine abdominal regions.
Listen to the intensity, pitch, and duration of the percussion note. Normally, tympanic sound produced by air in the bowel loops will be heard… As you percuss, watch the patient’s face for any signs of discomfort. Ask the patient if they are experiencing any tenderness. Tenderness on percussion is abnormal and can indicate peritoneal inflammation.
After abdominal area, percuss the lower anterior chest, above the costal margins. Dull sound on the right, over the liver is expected… On the left, one should hear tympany over the gastric air bubble and the splenic flexure of the colon… Following that, move to the area of pubic symphysis. Again, this should yield a tympanic sound…dullness indicates enlarged uterus or distended bladder.
Next step is to determine the liver span. Start by locating the right midclavicular line. Starting in the area of tympany below the umbilicus, lightly percuss in the right midclavicular line moving upwards… Make a mark where the tympany changes to dullness with a skin pencil. This is the lower border of the liver. Then, starting at the nipple line, again percuss in the right midclavicular line moving downwards. Note the point where the resonant sound changes to dullness…and mark it with a skin pencil. This is the upper border of the liver. Measure the distance between upper and lower border in centimeters. The liver span is normally 6-12 cm.
Following the liver span measurement, percuss to detect splenomegaly. The two maneuvers for this include Percussion of the Traube’s space and the Castell’s method. For percussion of the Traube’s space, make sure that the patient’s left arm is slightly abducted, and percuss from the medial to lateral border of this area. Overall dullness on percussion, or reduction of the area of tympany can indicate spleen enlargement. For the Castell’s method, percuss in the anterior axillary line in the lower intercostal space. Ask the patient to take a deep breath and percuss again. Normally, the percussion tone is tympanic on both inspiration and expiration. If the percussion note is dull, or becomes dull on inspiration, splenomegaly should be suspected.
Lastly, percussion is helpful to detect the cause of a protuberant abdomen. If the patient has a protuberant abdomen, percuss from the umbilicus in a lateral direction and with the skin pencil make a mark of the point where the tympanic sound changes to dullness. Then, ask the patient to roll on their side and repeat the percussion starting from the top and make a second mark when the tympanic sound changes to dull. If abdominal fluid were present, the level of dullness on the side would shift upwards toward the umbilicus, compared to the level of dullness in supine position.
You’ve just watched JoVE’s video on percussion to be performed during an abdominal exam. You should now know the important abdominal percussion steps and understand differential diagnoses that can be performed by proper interpretation of percussion findings. As always, thanks for watching!