In this report, the utility of MRM technique as a non-invasive modality to determine the structural and functional changes in the hearts of animals affected with EAM is shown. Myocarditis was induced in A/J mice by immunizing the animals with Myhc-α 334-352 in CFA7, and the animals were subjected to MRM experiments on day 21 post-immunization. The MRM imaging was performed on live animals under isoflurane anesthesia at 9.4 T (400 MHz for protons) using an 89 mm vertical-bore magnet equipped with triple axis gradients (maximum strength 100 G/cm). A scout image was acquired to locate and position the mouse heart in the center of the FOV, followed by axial images to obtain the long-axis 4-chamber view. The angle at which the heart was imaged for the 2-chamber view is shown in Figure 2A. Cardiac images were acquired using a 4 cm millipede RF imaging probe with a gradient-echo-based cine pulse sequence. Cardiac function measurements (imaging: LV wall thickness; output: LV end-diastolic volume and ejection fraction) were then analyzed using Segment software. Structural defects in the hearts of EAM-affected mice were evidenced by increase in LV thickness by approximately 1.5-fold (p = 0.018) (Figure 2B and Table 1), with corresponding decrease in LV end-diastolic volume [18.0 ± 4.2 µl vs. 37.5 ± 3.5 µl, Figure 2C(i); p = 0.002] and ejection fraction [49.4 ± 2.3% vs. 71.5 ± 6.0%, p = 0.00066; Figure 2C(ii)] as compared to healthy mice. As expected, histological evaluation of hearts from myocarditic, but not healthy, mice showed multifocal lymphocyte infiltrates, as we have demonstrated previously7; Figure 2D). The data suggest that morphological and functional changes in inflamed hearts can be non-invasively monitored by MRM in live animals.
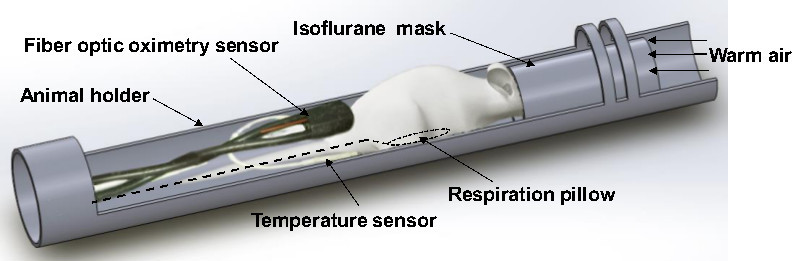
Figure 1. Animal preparation and positioning of probes for acquisition of MRM images from the mouse heart. To acquire images from the heart, the anesthetized mouse is placed in the animal holder specially designed for MRM imaging and connected to the air blow heater to maintain the body temperature. Under continuous anesthesia, the animal is immobilized in the prone position. A pneumatic pillow, fiber optic oximetry sensor and temperature sensor are set up to monitor respiration, pulse and body temperature, respectively, until MRM acquisition of cardiac images is complete. Please click here to view a larger version of this figure.
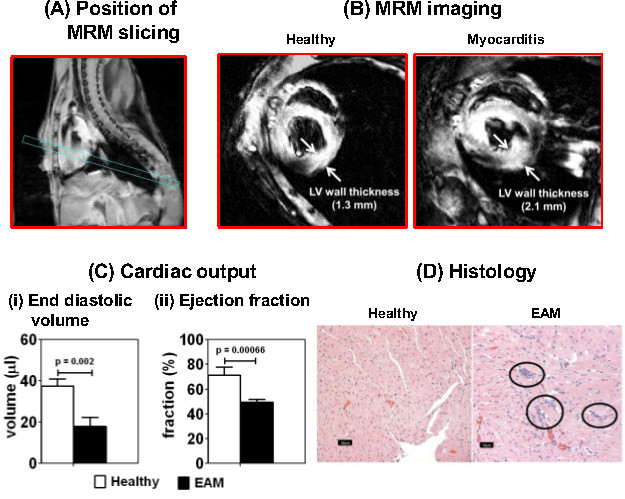
Figure 2. MRM imaging of mice affected with autoimmune myocarditis reveals cardiac abnormalities. Myocarditis was induced in A/J mice by immunizing the animals with Myhc-α 334-352 in CFA. The animals were subjected to MRM imaging on day 21 postimmunization to evaluate cardiac abnormalities. (A) Position of MRM slicing. The angle at which the heart was sliced for image acquisition is shown. (B) MRM imaging. Short-axis slices of heart were captured using echo-based cine pulse sequence in eight time frames with a TR of 500 msec (TE, 5 msec; flip angle, 20°; number of acquisitions, 4; acquisition matrix, 256 x 256) [arrows: LV wall thickness]. (C) Cardiac output. Cardiac output was measured based on (i) LV end-diastolic volume and (ii) ejection fraction in healthy and myocarditic mice using quantitative medical image analysis with Segment software. Mean SEM values for a group of mice are shown (n = 2 to 5 per group). (D) Histology. Hearts from the above treatment groups were evaluated for inflammation by hematoxylin and eosin staining. Circles: multifocal lymphocytic infiltrations. Please click here to view a larger version of this figure.
| Animals | Healthy (n = 3) | EAM (n = 5) |
| Mouse 1 | 1.03 | 1.48 |
| Mouse 2 | 1.3 | 1.59 |
| Mouse 3 | 0.94 | 1.44 |
| Mouse 4 | 2.11 | |
| Mouse 5 | 1.92 | |
| Mean ± SEM | 1.09 ± 0.1 | 1.71 ± 0.1 |
Table 1. Comparison of left ventricular (LV) wall thickness between healthy and experimental autoimmune myocarditis (EAM) mice. Three healthy and five EAM-induced mice were subjected to magnetic resonance microscopy (MRM) imaging on day 21 postimmunization. After acquiring the cardiac images by MRM, the thickness of LV wall was measured using Segment software as described in the protocol. The values displayed in the table represent LV wall thickness in mm.
