Here, a quantitative analysis of orofacial size and shape was demonstrated to compare embryos treated with a retinoic acid receptor inhibitor (RAR inhibitor) to untreated controls. Embryos were treated with a 1 μM concentration of this chemical inhibitor from stage 24 to 30 (26-35 hpf), washed out, and fixed at stage 42 (82 hpf). They were then processed and analyzed as described in the protocol. Results are original data, but consistent with observations in previous publications2,3. Control embryos were treated with the vehicle, DMSO, and developed normally (Figure 7Ai,ii). Embryos treated with a 1 μM concentration of the RAR inhibitor showed slight narrowing of the face, eye anomalies, and a malformed embryonic mouth opening that was more triangular shaped (Figure 7Aiii,iv).
First, traditional orofacial dimensions were measured and are summarized in Figure 7B. Statistical significance was determined by performing a Student’s t-test assuming unequal variance between inhibitor treated embryos and controls for each measurement. We found that both snout length and face width were significantly decreased in RAR inhibitor treated embryos compared to controls (p-values = 0.0062 and 0.0058, respectively; Figure 7Bi,ii). While face height and mouth roundness were significantly increased (p-values = 3.7772 x 10-6, 1.4812 x 10-7), mouth width was significantly decreased (p-value = 2.5175 x 10-10; Figure 7Biii-v).The results showed no significant difference in the overall orofacial area between the two groups (p-value = 0.3754; Figure 7Bvi). These data show that loss of retinoic acid signaling at a specific time in development results in a shorter snout, slight narrowing of the midface region, and malformation of the embryonic mouth opening.
To provide a sophisticated view of the shape changes of the embryonic orofacial region in response to reduced retinoic acid signals, we next utilized geometric morphometric analyses. After identifying and aligning orofacial landmarks using morphometric analysis software, we then examined the variance within each group via principal component analysis (PCA). When the first two principal components were plotted against each other, RAR inhibitor treated embryos were clearly distinguished from controls along the PC1 axis (Figure 7C). This test also showed the outliers in the sample set- illustrated by two inhibitor treated embryos that did not cluster with the rest of the group (Figure 7C, arrows).
Next, the statistical differences in the shape of the orofacial region between RAR inhibitor treated embryos and controls were assessed and visualized by performing a discriminant function analysis (DFA). The Procrustes distance between the two groups was significantly different (distance = 0.2665, p-value < 0.0001, Figure 7D), indicating a change in orofacial shape when retinoic acid signaling is disrupted. Indeed, dramatic shifts in the position of lateral landmarks in the orofacial region indicate a narrowing of the face shape respective to the height in inhibitor treated embryos (Figure 7D). In addition, the slight outward shift in position of the nasal landmarks (Figure 7D, arrows) reveals the abnormality in nostril position in these embryos that is consistent with decreased outgrowth of the snout. The shifts in landmarks that define the edges of the mouth opening show position changes that reflect the formation of a triangular shaped mouth opening that is consistent with the median cleft reported in our previous studies 2,3. In addition to vector shifts, the warping pattern of the transformation grid also illustrates shape changes in the orofacial region. Warping in the midface region is consistent with the midface hypoplasia and overall facial narrowing seen in embryos with decreased retinoic acid signals (Figure 7D).
The results of the discriminant function analysis (DFA) show shape changes that were consistent with our qualitative analysis, as well as revealing some changes that were not adequately captured by traditional size measurements alone. For instance, while the orofacial area was not significantly different between controls and inhibitor treated embryos (Figure 7Bvi), the DFA transformation grid revealed dramatic changes in this region consistent with the facial narrowing seen in inhibitor treated embryos (Figure 7A,D). Further, the warping pattern and landmark shifts of the mouth opening, coupled with the significant change we saw in mouth roundness, illustrate the malformation of the mouth opening shape in inhibitor treated embryos. In summary, a combination of traditional measurements of facial dimensions and geometric morphometric analysis illustrates the changes in shape and size of the orofacial region when retinoic acid signals are disrupted.

Figure 1. Required materials. (A) Tools for data analysis. (i) 24-well plate, (ii) standard disposable transfer pipette, (iii) Dumont #5 Inox forceps, (iv) clay-lined Petri dish, (v) straight teasing needle, (vi) glass pipette tool, (vii) sterile, disposable scalpel. (B) Preparation of the clay-lined dish. (i) A straight teasing needle is used to draw horizontal lines in the clay. (ii) A glass pipette tool is used to make circular depressions along each row. (iii) The dish is filled with PBT for imaging.

Figure 2. In vitro fertilization and culture of Xenopus eggs. (A) Following HCG injection, adult Xenopus laevis females are induced to lay eggs. (B) Eggs are collected in high salt MBS, fertilized with testes extracted from a male, and cultured using standard methods. (C) Embryos are transferred to a 24-well dish containing 0.1x MBS using a standard, disposable transfer pipette. (D) A calibrated pipette-man is used to measure 1 ml into an empty well, and a marker is used to demarcate this level on the outside of all wells containing embryos (inset). 0.1x MBS is then added or taken away so that it is level with this mark.

Figure 3. Preparation of embryo heads for imaging. (A) Diagram of the two incisions required to remove heads, solid black lines. Scale bar = 400 μm. (B) The first incision is made at the posterior end of the gut to remove the tail and release pressure from the scalpel. Scale bar = 400 μm. (C) The second incision is made at the anterior end of the gut, near the heart, to completely sever the head. Scale bar = 400 μm. (D) Frontal views of row of embryo heads positioned in clay. Scale bar = 650 µm. (E) Lateral views of row of embryo heads position in clay. Scale bar = 500 µm cg: cement gland.

Figure 4. Traditional size measurements of orofacial dimensions. (A) Face width. Arrows indicate the points where the ventral portion of the eye meets the periphery of the face. Red line is the face width, measured as the distance between these points. Scale bar = 210 µM. (B) Face Height. White lines are guides drawn prior to measurement at the dorsal edge of the eyes and the dorsal edge of the cement gland. Red line is the face height, measured as the distance between these two guides at the midline of the face. Scale bar = 210 µM. (C) Orofacial area. White lines are guides drawn prior to measurement. (a) Point where the bottom guide meets the ventral edge of the left eye. Red line shows the tracing around the left eye. (b) Point where the dorsal edge of the eye meets the top guide. Blue line shows the dorsal boundary of orofacial area, traced along the top guide at the dorsal edge of the eyes. (c) Point where the top guide meets the right facial periphery. Green line shows the tracing around the right eye. (d) Point where the ventral edge of the right eye meets the bottom guide. Yellow line shows ventral boundary of orofacial area, traced along the bottom guide at the dorsal edge of the cement gland. Scale bar = 210 µM. (D) Snout length. White line is the anterior edge of the eye and is drawn as a guide prior to measurement. Red line is snout length, measured from this line to the point where the dorsal edge of the cement gland meets the lateral periphery of the face. Scale bar = 300 µM. (E) Mouth width. Arrows are the points where the dorsal and ventral lips meet. The red line is the mouth width, measured as the distance between these two points. Scale bar = 200 µM. (F) Mouth roundness. The perimeter of the mouth opening is traced and shown in red. cg: cement gland. Scale bar = 200 µM.
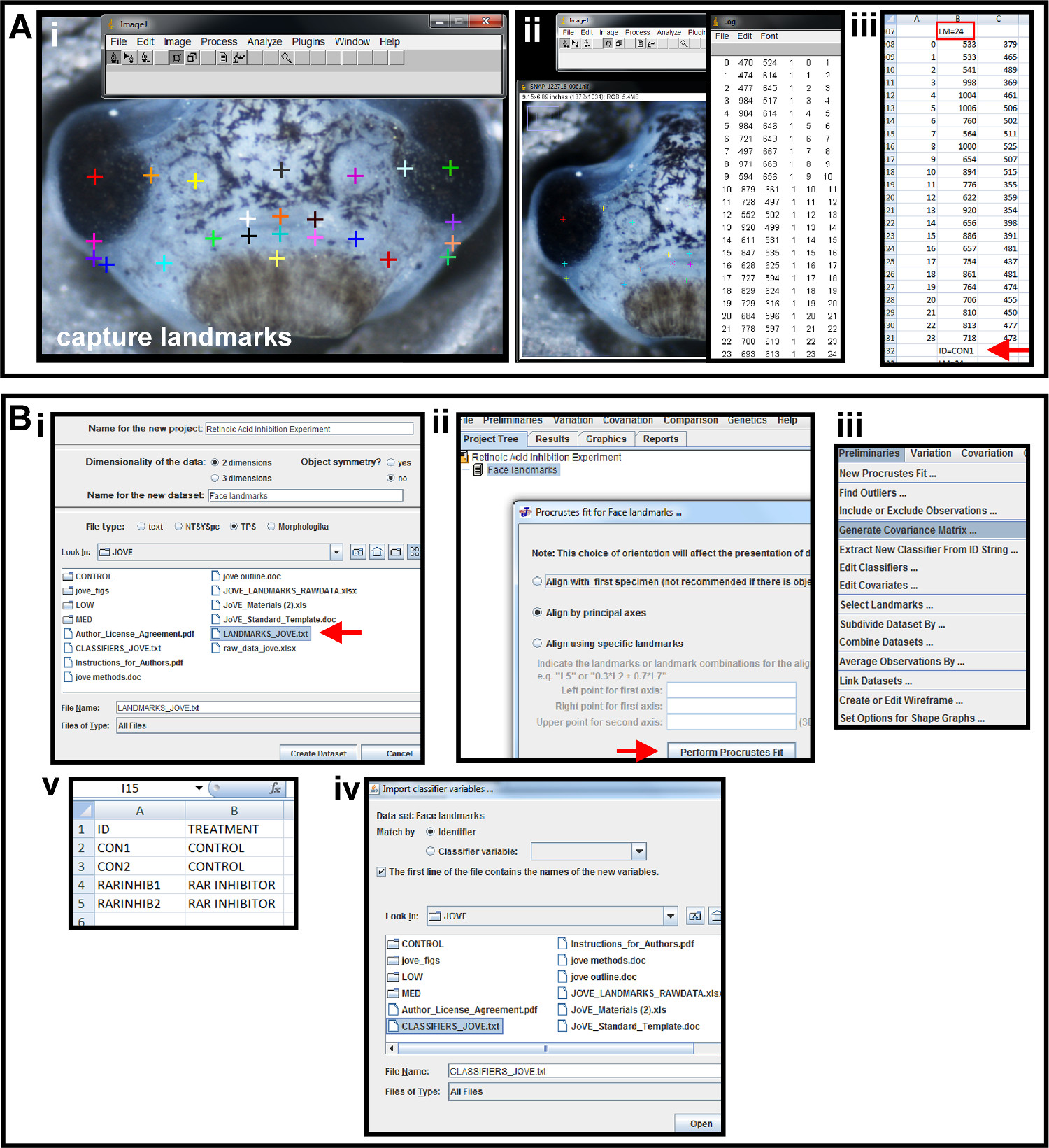
Figure 5. Capturing landmarks and preliminaries for geometric morphometric analysis. (A) Using photo-editing software and a spreadsheet program to place landmarks and capture coordinates. (i) Multicolored crosses are the landmarks placed on the image using the Add points tool in ImageJ to represent the shape of the orofacial region. (ii) Landmark data is displayed by using the Display Results Tool. (iii) Landmark data is copied and pasted into a spreadsheet. Above the second column is a header identifying the number of landmarks and denoted by "LM=24" (red box). Below the second column of data, the sample is given a unique name and denoted by "ID=CON1" (red arrow). This is repeated for all images in a sample set and the data is saved as a text file. (B) Preliminary data analysis in a geometric morphometric software program. (i) The text file created in from the photo-editing software is imported into the morphometric program, MorphoJ, as a TPS file. File is indicated by red arrow. (ii) Landmark coordinate data is aligned by Procrustes fit by principal axes. Red arrow indicates execution of alignment. (iii) A covariance matrix of Procrustes fit landmarks is generated in the Preliminaries menu. (iv) A classifier file is created in a spreadsheet. Column A and B are given headers “ID” and “TREATMENT”, respectively. The ID’s given to each sample in landmark data collection are input under column A, and the treatment group to which each sample belongs is input in column B. (v) The classifier file is imported into the morphometric program as a classifier variable set and Matched by Identifier for the chosen data set. Please click here to view a larger version of this figure.
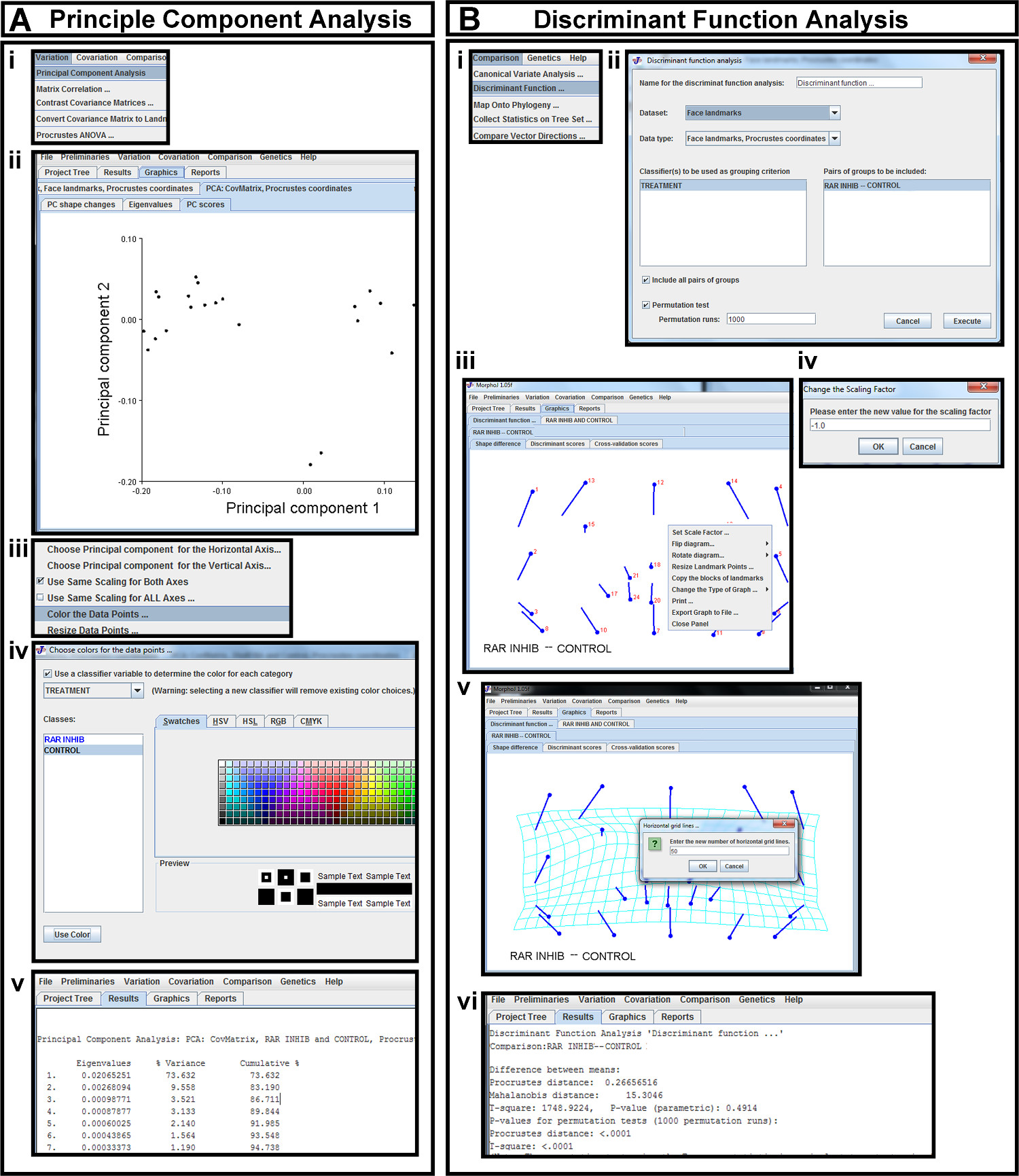
Figure 6. Statistical analysis in morphometric software. (A) Principal Component Analysis (PCA) (i) PCA is selected from the Variation tab. (ii) The first two principal components of Procrustes landmarks are displayed as a scatterplot in the PC scores tab. (iii) A pop-up menu is brought up in the plot space. This menu is used to change which principal components are plotted against each other (red arrow) and to color the data points (highlighted in blue). (iv) The data points are colored according to the classifier variables in the pop-up menu. (v) Percentage of variance captured by each principal component is viewed in the Results tab. (B) Discriminant Function Analysis (DFA) (i) DFA is selected from the Comparison tab. (ii) The data set of Procrustes coordinates is selected for DFA, and the previously uploaded classifiers are chosen for grouping. The desired groups to be compared are chosen and permutation tests are run. (iii) DFA results are displayed as a vector map in the Shape Difference tab. A pop-up menu in the plot space can be used to orient the image correctly. (iv) By selecting the Set Scale Factor tab in the pop-up menu, the sign of the scale factor can be changed. (v) The vector map is changed to a transformation grid with the desired number of grid lines by choosing Change the Type of Graph in the pop-up menu of the vector map. (vi) The Mahalanobis and Procrustes distances and corresponding p-values are viewed under the Results tab. Please click here to view a larger version of this figure.
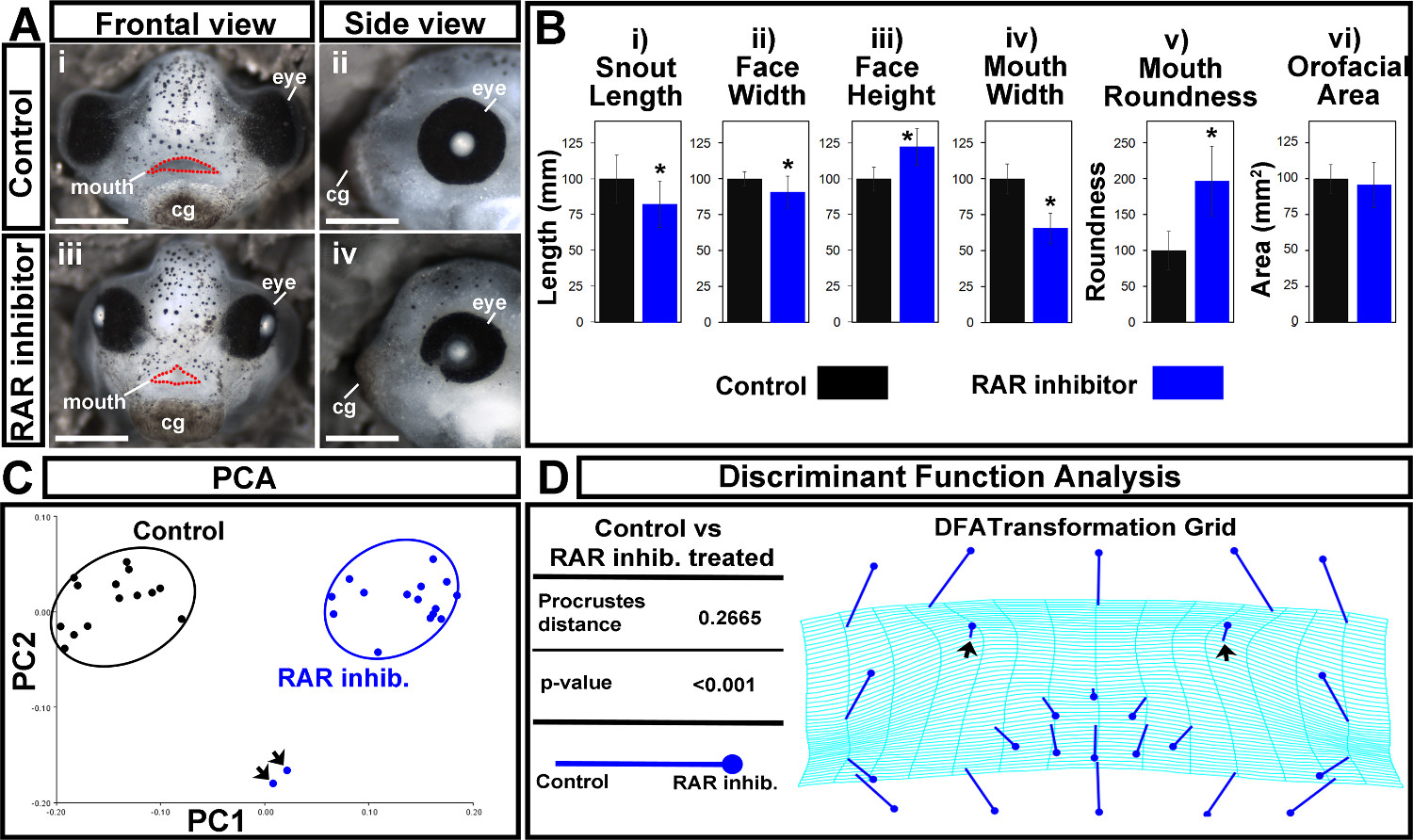
Figure 7. Orofacial analysis of control and RAR inhibited treated embryos. (A) (i,ii) Representative images of controls. Scale bars = 270 µm. (iii,iv) Embryos treated with a 1 μM concentration of the RAR inhibitor, BMS-453. Scale bars = 260 µm. (i,iii) Frontal views. Mouth opening is outlined in red dots. (ii,iv) Side views. cg: cement gland. (B) Traditional orofacial dimensions of control (black) and inhibitor treated (blue) embryos. (i) snout length, in mm (ii) face width, in mm (iii) face height, in mm (iv) mouth width, in mm (v) mouth roundness, a unit-less number determined in ImageJ using the equation: (4 × [Area]) / (π × [Major axis]2). (vi) Orofacial area, in mm2. Asterisks indicate significance as determined by Student’s T-test assuming unequal variance. α < 0.05. (C) Principal Component Analysis. Controls are in black and RAR inhibitor treated embryos are in blue. Black arrows indicate outliers. PC1 = 73.63%, PC2 = 9.56%. (D) Discriminant Function Analysis displaying the Procrustes distance and p-value, in addition to a transformation grid. Closed circle end of vector is landmark position in RAR inhibitor treated embryos. The end of the line of the vector is the landmark position in controls. Black arrows indicate shift in nasal landmarks. Please click here to view a larger version of this figure.
