This procedure typically lasts 2-2.5 hr. The patients are under deep analog-sedation, meaning that they are sleeping, receiving analgesics but breathe spontaneously. If all endpoints including bi-directional block in all pulmonary veins, healthy left atrial tissue, and non-inducibility of atrial fibrillation or atrial flutter are achieved, patients have about a 75% probability of freedom from atrial fibrillation recurrence after 12 months. If the left atrium has fibrotic tissue with low voltage areas (see Figure 2), the chances of permanent freedom from arrhythmias decrease compared to patients with healthy left atrial tissue (see Figure 3). Typically, patients can be discharged 24 hr after the procedure. In the first 4-6 weeks after the ablation procedure, short episodes of atrial arrhythmias can occur and are frequent. After 6 weeks, the likely outcomes of the ablation procedure are evident. In most cases, all medical anti-arrhythmic treatments are discontinued on the day of the ablation procedure. Oral anticoagulation is mandatory and needs to be continued after the ablation procedure irrespective of the individual’s stroke risk for at least 3 months.

Figure 1: Ablation of atrial fibrillation using NFCV technology. Left and middle: catheter visualization using the NFCV technology: ablation catheter (red tip) in the left superior pulmonary vein (LSPV, blue marker). Right: the same setting displayed in the 3D mapping system. Ablation catheter (green halo) placed in the left superior pulmonary vein close to the ridge to the left atrial appendage. Esophageal temperature probe posterior to the left atrium (green catheter). Please click here to view a larger version of this figure.

Figure 2: Voltage map of a “diseased” left atrium. 3D reconstructed CT with low-voltage areas at the posterior wall of the left atrium and in the mitral isthmus region indicating areas of previous ablation. Please click here to view a larger version of this figure.

Figure 3: Voltage map of a “healthy” left atrium. 3D reconstructed CT model of a left atrium. A color-coded voltage map is shown with purple for healthy tissue (electrograms >0.5 mV) and grey for scar tissue (electrograms <0.2 mV). Electrogram amplitudes >0.2 mV and <0.5 mV are displayed in yellow, red, and blue. Please click here to view a larger version of this figure.
Video 1: Principle of NFCV. In the beginning of the procedure, 2 short cine loops (3 sec each) are recorded and are used as the dynamic background for catheter visualization. Specially-designed catheters with miniaturized sensors at the tip are inserted in the patient and visualized by the NFCV system. Please click here to view this video.
Radiation exposure for interventional cardiologists and electrophysiologists is an underestimated risk because of its unpredictable side-effects. Current literature reveals a higher incidence of left-sided brain-tumors among this subgroup of clinicians, suggesting that the proximity of the left hemisphere to the X-Ray source may be a culprit12. The latency between radiation exposure and diagnosis of neoplasia has been reported to be 20 years or more. Therefore, today’s interventionalists should use all technological options to reduce radiation exposure to a minimum.
The NFCV system can help reduce fluoroscopy exposure without affecting procedure time14,15 with a workflow that was adapted several times over the past 3 years in order to minimize radiation exposure according to the ALARA principle.
3D mapping systems can help to improve the understanding of complex 3-dimensional structures, but the basic orientation for the operator is generated using conventional fluoroscopy.
The transseptal puncture remains the largest contributing step (75-80%) of the radiation dose during these procedures since no sensor-equipped material for use with NFCV technology is currently available. Especially in unexperienced hands this represents the most critical step in that procedure- other imaging modalities (such as intracardiac or transesophageal echo) can contribute to safe punctures and low complication rates.
The NFCV is not only used in ablation procedures but also in complex implantations such as cardiac resynchronization therapy (CRT). In these procedures, the system allows the reduction of fluoroscopy burden by 75-80% compared to conventional implantations13. A recent publication could show that after a learning curve of 30 – 40 procedures a median fluoroscopy time of 1.1 min for 50 consecutive patients is feasible and safe14. This was confirmed when extending the data acquisition to >500 patients (see Figure 4).
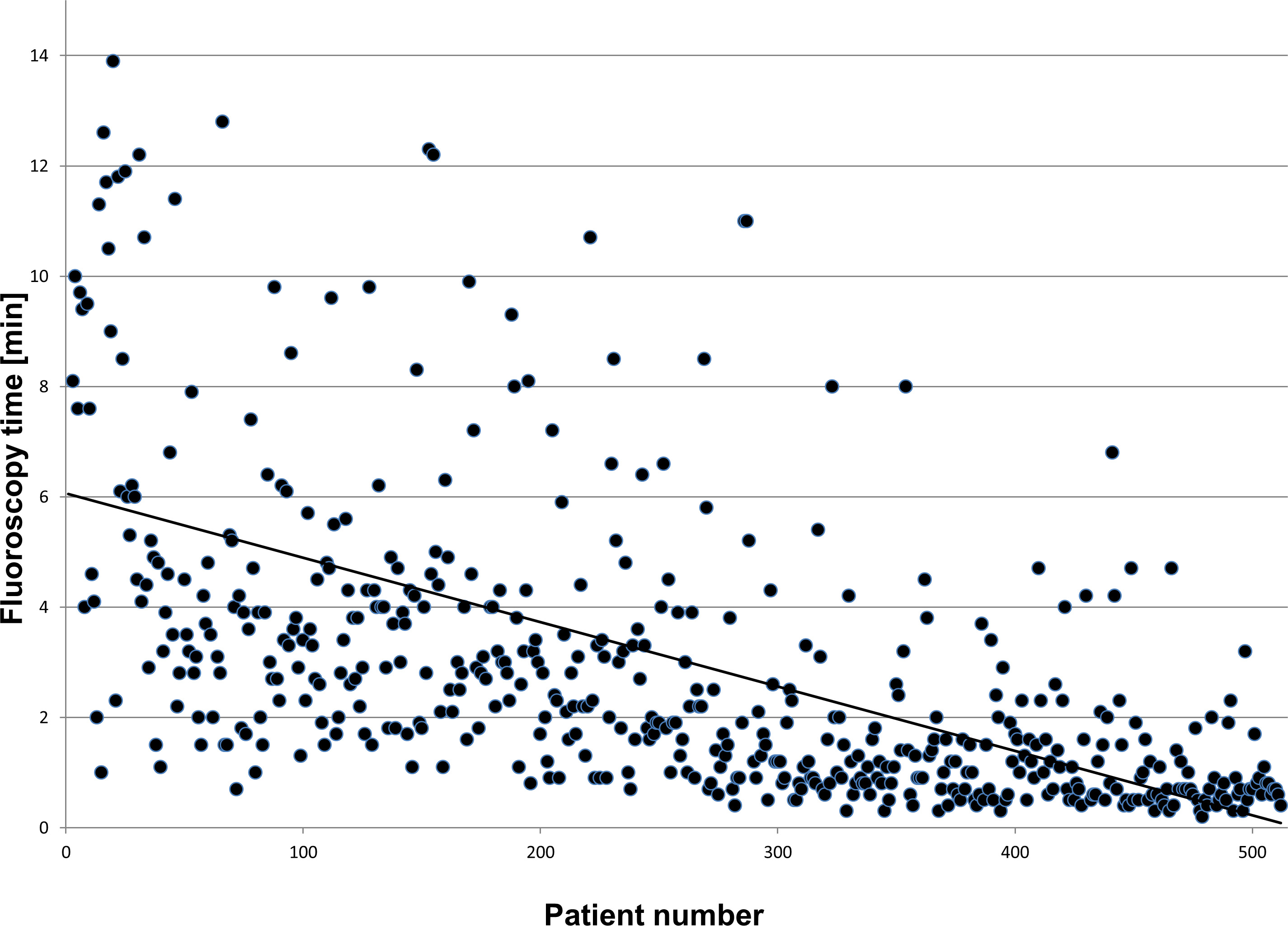
Figure 4: Please click here to view a larger version of this figure.
The limitation of the current available system is that only the tips of the catheters are visualized. Unexperienced operators will probably not be able to interpolate from the orientation of the tip to know what the position of the catheter shaft will be. Furthermore, the system is not able to visualize the transseptal sheath yet. Only a limited choice of catheters are currently available- therefore only a limited number of different procedures is suitable using NFCV technology.
In near future more devices and tools will be available that are equipped with a sensor to be visualized non-fluoroscopically. The system here basically works as a cardiovascular platform for different procedures; electrophysiology is just the first application that has been introduced.
