

Summary
The topical anesthetic lidocaine was atomized using a high oxygen flow through the working channel of a flexible intubating endoscope to achieve topical airway anesthesia for awake endotracheal intubation. We prefer this modified spray-as-you-go technique for endoscopic intubation to classical bolus application because of higher patient satisfaction and better compliance.
Abstract
A patient's willingness to cooperate is an absolute precondition for successful awake intubation of the trachea. Whilst drug-sedation of patients can jeopardize their spontaneous breathing, topical anesthesia of the airway is a popular technique. The spray-as-you-go technique represents one of the simplest opportunities to anesthetize the airway mucosa. The application of local anesthetic through the working channel of the flexible endoscope is a widespread practice for anesthetists as well as pulmonologists. There is neither need for additional devices nor special training as a pre-requisite to perform this technique. However, a known clinical problem is the coughing and gagging reflex that may occur when the liquid anesthetic strikes the airway mucosa and other sensitive structures like the vocal cords. This can be avoided by the use of oxygen applied through the working channel with the aim of fogging the local anesthetic into finer particles. Furthermore, the oxygen flow provides a higher oxygen supply and contributes to a better view, dispersing mucus secretions and blood away from the lens. Using an atomizer with a high oxygen flow of 10 L/min we maximized these benefits, caused less coughing and had more satisfied and therefore cooperative patients. Possible, but very rare complications of using oxygen flow including gastric insufflation, organ rupture or barotrauma did not arise. We attribute the complication-free use of high oxygen flow to the design of the set, which permits flow and pressure release.
Introduction
Topical anesthesia of the airway for awake intubation is generally recommended to improve patient comfort, which will help make the procedure a success. The spray-as-you-go technique with high oxygen flow is a simple and safe concept that is finding a high level of acceptance among patients. The atomization of the local anesthetic by oxygen at a flow rate of 10 L/min results in less stimulation of the cough and gag reflex.
Faced with negative feedback from several patients, we decided to refine the standard institutional spray-as-you-go technique. This classical bolus application of local anesthetic consisted of two injections, each of 5 mL lidocaine 2% plus 5 mL air in a 10 mL syringe, first into the vocal cords and then, after a 2-min waiting time, into the trachea. Patients complained about the feeling of being drowned by the splash of the bolus striking their airway mucosa.
The spray-as-you-go technique is commonly used worldwide1. This technique involves local anesthetic application through the working channel of a flexible intubating endoscope while advancing the tip through the upper and lower airway with the goal of intubating the patient´s trachea. There are multiple approaches in practice and several descriptions of methods in the literature. Initial experiences with the spray-as-you-go-technique in combination with application of a constant oxygen flow through the working channel were published in the 1990s2. The focus here was on oxygen flow effects like cleaning the lens by dispersing mucus secretions and blood away from the lens and elevating the inspiratory oxygen delivery. The advantage of the oxygen flow in aiding atomization of local anesthetic was shown previously by Piepho and colleagues3. They described a vaporization technique, where the supply of 3 L/min oxygen resulted in less coughing by the patients. On the assumption that a flow of 10 L/min would atomize the local agent into finer particles that would evoke even less coughing, we successfully tested the atomizer at this higher flower rate. The atomizer consists of a small volume, kink-resistant, flexible, pressure-certified oxygen tube and a connecting tube. These are connected to a three-way sidearm fitting with a small flow-control opening.
The atomizer technique can be used for all airway situations. However, the device should be used cautiously distal from higher-grade airway stenosis caused by conditions such as tumor masses. The lack of backflow of oxygen could cause increased airway pressure and increases the risk of barotrauma. Also, the atomizer is a useful tool in an emergency setting. The preparation of the set needs less than a minute and the user needs no special training. In the following we present detailed operating instructions for the spray-as-you-go technique with high oxygen flow, illustrating the separate working steps.
Subscription Required. Please recommend JoVE to your librarian.
Protocol
All procedures were approved by the ethics committee of the medical association of the State Rhineland-Palatinate and performed in accordance with the Declaration of Helsinki.
1. Atomizer4
- Remove the set from package. Inspect the product to ensure there is no damage.
NOTE: The device is intended for one-time use. Please refer to the instructions for use for further information about storage and supply (see Materials and Equipment Table).
2. General Preparation of the Patient
- Administer premedication, e.g. Lorazepam 1 - 2.5 mg the evening before and/or 2 - 4 mg 1 - 2 h before the intervention (with attention to contraindications).
- Establish monitoring parameters such as pulse oximetry (SpO2), electrocardiography (ECG) and non-invasive blood pressure (NIBP).
NOTE: Monitor patient sedation using standards such as Ramsay Sedation Scale and Bispectral Index monitoring. Close monitoring of the level of sedation can help prevent potential complications such as respiratory depression. - Secure a peripheral intravenous access.
3. Topical Anesthesia of the Upper Airway
- Apply 1 mL mixture of lidocaine 2% with phenylephrine 0.25% to each nostril.
- Apply lidocaine 10% spray twice directly onto the mucosa of the oropharynx, spraying from the tip to the back of the tongue. Ask the patient to gargle the lidocaine in the mouth for as long as possible.
NOTE: Anesthesia of the supraglottic airway can be performed alternatively using cotton-tipped swabs or nasopharyngeal airways, drops, gel, swish and gargling, aspirating and spraying local anesthetics.
4. Analgo-sedation
- Start analgo-sedation using i.v. medication, e.g. initial sufentanil bolus (< 60 kg: 5 µg; > 60 kg: 10 µg; > 100 kg: 15 µg).
NOTE: Dose drug-induced sedation at the lowest level possible in order to prevent apnea or airway constriction. - Give an extra sufentanil i.v. bolus, e.g. 5 µg, as 'rescue' treatment until a Ramsay Sedation Score of 2 (cooperative, oriented, tranquil) is achieved.
5. Equipment Preparation
- Assemble and check the flexible intubation endoscope according to institutional standards.
- Connect the oxygen tube of the atomizer to the oxygen flow meter directly.
Caution! Oxygen flow meters with humidifier bottles must not be used. - Attach the connecting tube to the Luer on the working channel of the endoscope. Set the oxygen flow rate to 10 L/min, as recommended in the instruction manual.
- Connect a 1 mL syringe containing the lidocaine 2% solution to the three-way sidearm fitting.
NOTE: Lidocaine 2% with its favorable efficacy profile is a suitable anesthetic.
6. Atomizer Technique
- Close the flow-control opening using a finger. Rapidly inject the medication. Immediately release the flow-control opening.
NOTE: A syringe must be connected to the three-way sidearm fitting to obtain a continuous low oxygen flow through the working channel. - While advancing the flexible endoscope in the airway, inject the local anesthetic using the atomizer at the following sites: inside nostril, on posterior nares; epiglottis; glottis; and vocal cords.
- Repeat these steps as often as required while advancing the endoscope ("spray-as-you-go"). Before passing through the vocal cords, wait for 2 min to allow sufficient drug effect at the site.
NOTE: Monitor sedation level of patient and top up sedation using i.v. medication (e.g. sufentanil 5 µg), as needed.
7. Flexible Endoscopic Intubation
- Advance the endoscope carefully through the glottis into the trachea and position the tip of the endoscope just above the carina. Railroad a suitable sized, cuffed and lubricated flexible endotracheal tube over the endoscope into the trachea under rotation.
NOTE: Avoid accidental advancement of the endoscope tip into a main stem bronchus. - Confirm placement of the endotracheal tube in the trachea just above the carina by visual control via the endoscope. Remove the endoscope, leaving the endotracheal tube in place.
- Confirm the endotracheal position of the tube by measuring end tidal CO2 using capnography in the spontaneously breathing patient.
- Induce general anesthesia, e.g. intravenous Propofol 2 mg/kg/body weight. Start ventilating the patients according to current standards.
NOTE: The Enk Atomizer set is currently not available from Cook Medical.
Subscription Required. Please recommend JoVE to your librarian.
Representative Results
We performed awake flexible endoscopic intubation using the presented topical anesthesia technique in 48 patients. We succeeded in intubating all patients except one, who suffered from a stenosing tumor of the pharynx, which made it impossible to advance the tube.
The quality of awake intubation comfort was evaluated by patients, anesthetists and nurses using an 11-point visual analog scale (VAS) from 0 = not unpleasant to 10 = intolerable. The atomizer technique met with broad acceptance, and the evaluation of comfort showed good performance. On the first postoperative day, patients rated their level of comfort with a median (Interquartile range (IQR)) VAS score of 1 (1 - 3). Anaesthetists and nurses rated the technique as VAS 2 (1 - 4 and 1 - 3 respectively).

Figure 1: Comfort level of patients undergoing awake endoscopic intubation on the first postoperative day, and comfort evaluation by anesthetists and nurses. VAS 0 = Not Unpleasant, VAS 10 = Intolerable. Symbol, Median; Error Bars, IQR. Please click here to view a larger version of this figure.

Figure 2: The median number of coughs in a control group, using the classical bolus application of 2 x 5 mL 2% lidocaine was nearly twice as high.
The incidence of coughing is a surrogate measure of the quality of awake-intubation. A trained and skilled study nurse, who was not involved in patient treatment at any time, exclusively collected data during the procedure to avoid reporting bias. We evaluated coughing when topical anesthesia was applied (protocol includes five injections of lidocaine). The median number of coughs during the period of intubation was 6 (3 - 10).
Further criteria used to evaluate the safety of awake-intubation were the time required for intubation and the consumption of local anesthetic in relation to neurological toxicity. The mean duration of awake-intubation was 5 (3 - 6) min. This period included the time required to administer the topical anesthetic using the atomizer. The atomized sprays could be administered one after another (spray as you go). Under the assumption that the atomized lidocaine penetrates deeper into the airway mucosa and for this reason acts faster, the protocol included only a 2-min waiting time before passing through the vocal cords.
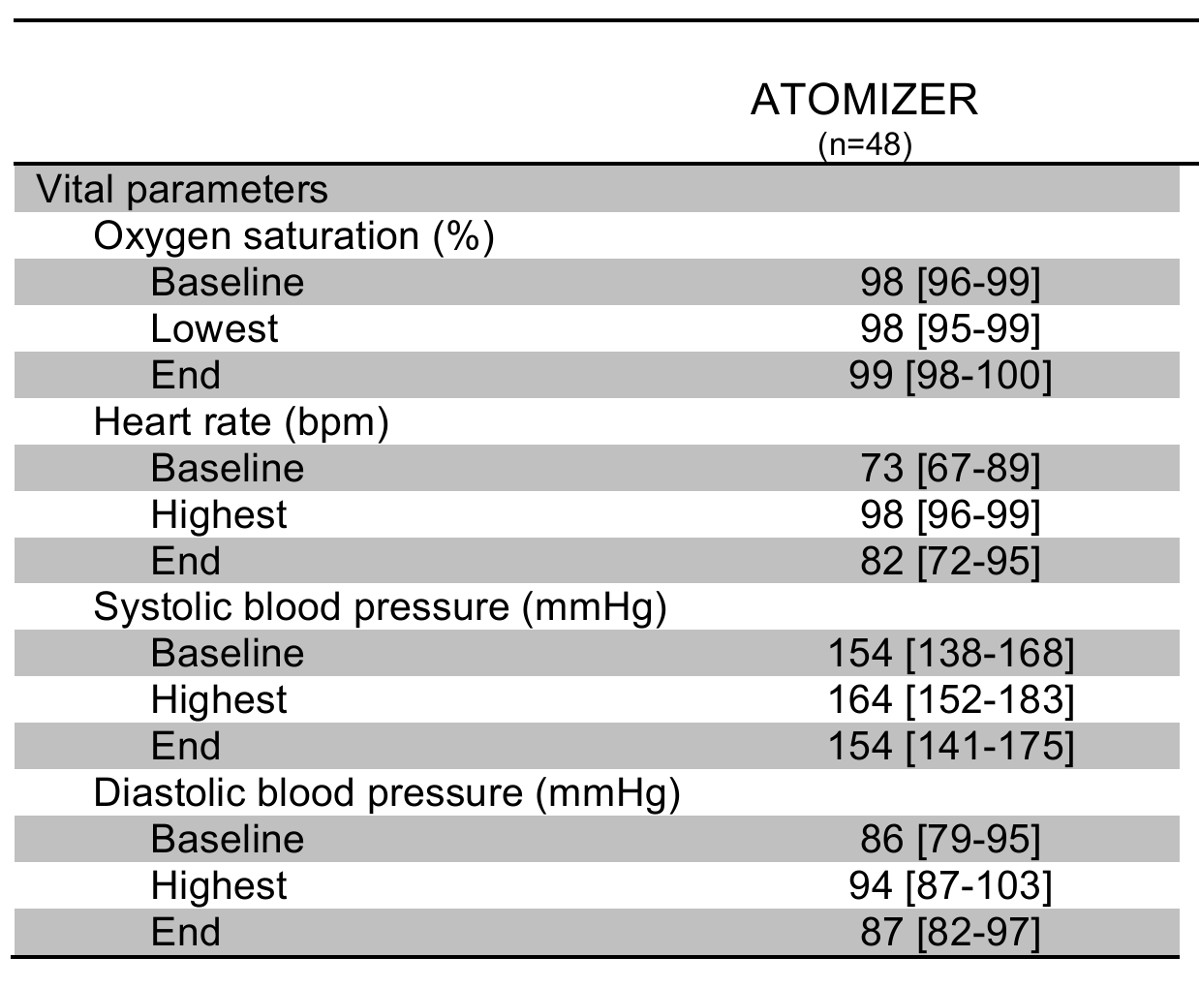
Use of the atomizer with a high oxygen flow led to a widespread distribution of local anesthetic. The average consumption of lidocaine 2% using the atomizer technique was 100 mg. The cardiovascular stability was probably a result of effective topical airway anesthesia in combination with an acceptable sedation protocol.

Table 1: Stability of the cardiopulmonary indices from the initiation of topical anesthesia to immediately after insertion of the endotracheal tube. Data were documented at baseline and every min thereafter. Data show median and IQR. Please click here to download this file.
Subscription Required. Please recommend JoVE to your librarian.
Discussion
Here we demonstrate topical anesthesia using an atomizer with high oxygen flow for awake-endoscopic intubation. The first study to evaluate the atomizer technique compared it with classical boluses of topical anesthesia via the working channel of the flexible intubating endoscope5. Patients in the atomizer group evaluated their level of comfort as better than those in the control group and experienced fewer coughs and distinct coughing episodes. In addition, the atomizer technique was faster and less local anesthetic was required.
When investigators compared the atomizer, using low oxygen flow, with translaryngeal injection for awake-intubation in patients at risk of cervical spine injury, there were no differences between the groups in terms of comfort evaluation6. The spray-as-you-go technique with high oxygen flow is one variation of several different described spray-as-you-go techniques.
A major advantage of all spray-as-you-go techniques is their flexibility, involving selectively and repetitively anesthetizing the airway, which makes these techniques a suitable choice for most endoscopic intubations.
The classical bolus application of local anesthetic regularly evokes patient discomfort. Several efforts have been made to reduce this limitation. For example, the use of an epidural catheter cut to the length of the flexible intubating endoscope and inserted through the working channel is repeatedly recommended in the literature7,8,9. The outcome of this modification has not yet been confirmed due to the lack of prospective, controlled and randomized studies. However, a limitation of the epidural catheter technique is that an experienced operator is needed to successfully maneuver the local anesthetic application. Additionally, using an epidural catheter for local anesthetic application was reported to be costly and time consuming8,10.
An additional advantage of the spray-as-you-go technique is its ease of handling. Nebulization of local anesthetic requires additional equipment (e.g. ultrasonic nebulizer) and additional time prior to endoscopic intubation. Furthermore, the spray-as-you-go technique can be used for almost every patient, while a cooperative patient and knowledge of anatomy and the identification of landmarks are fundamental requirements when performing an airway nerve block.
Intra-arterial injection, hematoma formation and tracheal injury such as subcutaneous emphysema are feared complications due to the invasiveness of performing blocks, but complications caused by the spray-as-you-go technique are rare.
Potential complications of using a constant oxygen flow (3 to 5 L/min) through the working channel of an intubation endoscope include gastric insufflation and organ rupture11,12,13. Complications may occur during difficult visualization of airway structures, a prolonged procedure or accidental esophageal intubation. Barotrauma of the lung is theoretically possible if the intubation endoscope is passed through a narrowed glottis and passage of the tracheal tube is delayed because of a narrowed airway. For these reasons, some authors do not recommend applying oxygen through the working channel of an intubation endoscope14. None of the above-mentioned complications was observed in the two studies investigating the atomizer5,6. This could be attributed to the flow-control opening of the atomizer, a 2 mm hole placed opposite the injection port of the three-way-sidearm fitting, which allows flow and pressure release if no injection is performed. It is assumed that there is no continuous high oxygen flow and pressure at the distal end of the working channel of the endoscope, because oxygen can escape through the flow-control opening. Only at the time of injection, when it is closed, might the subsequent airway structures be under a higher pressure.
There are no data on the pressure at the distal tip of the endoscope working channel when administering oxygen or the distribution and penetration depth of local anesthetic on, and in, the airway mucosa. This, as well as the mechanism as to how high flow oxygen atomizes local anesthetic, would be worth investigating.
Subscription Required. Please recommend JoVE to your librarian.
Disclosures
The authors have nothing to disclose. The Enk-Atomizer set is currently not available from Cook Medical. According to the inventor (personal communication) a comparable device will be available in the future.
Acknowledgments
The authors have no acknowledgements.
Materials
| Name | Company | Catalog Number | Comments |
| Lidocaine 10% pump spray | e.g. AstraZeneca | ||
| Opiod for i.v. administration | Any opiod can be used. We prefer either Sufentanil or Fentanyl | ||
| Enk Fiberoptic Atomizer Set | Cook Medical | C-EFNS-100 | The Enk Atomizer set is currently not available from Cook Medical |
| Lidocaine 2% | e.g. AstraZeneca | ||
| Intubation endoscope | e.g. Karl Storz Endoscope | We prefer a fibrescope with an outer diamter of 5 mm and a working channel with a diamter of 2 mm | |
| Endotracheal tube | e.g. Rüsch | Size of the endotracheal tube needs to be adjusted to the patient. We prefer a ID 6.5 mm for nasal approach and ID 7.0 mm for oral approach | |
| Anesthetic drug, e.g. Propofol 1% | e.g. AstraZeneca |
References
- Simmons, S. T., Schleich, A. R. Airway regional anaesthesia for awake fibreoptic intubation. Reg Anesth Pain Med. 27, 180-192 (2002).
- Benumof, J. L. Management of the difficult adult airway. With special emphasis on awake tracheal intubation. Anesthesiology. 75, 1087-1110 (1991).
- Piepho, T., Thierbach, A. R., Göbler, S. M., Maybaur, M. O., Werner, C. Comparison of two different techniques of fiberoptic intubation. Eur J Anaesthesiol. 26, 328-332 (2009).
- Cook Incorporated, Atomizer instructions for use. , Available from: www.cookmedical.com/data/IFU_PDF/C-T-EFNS1004.PDF (2004).
- Pirlich, N., Lohse, J. A., Schmidtmann, I., Didion, N., Piepho, T., Noppens, R. R. A comparison of the atomizer with boluses of topical anaesthesia for awake fibreoptic intubation. Anaesthesia. 71, 814-822 (2016).
- Malcharek, M. J., et al. Comparison of the Enk Fibreoptic Atomizer with translaryngeal injection for topical anaesthesia for awake fibreoptic intubation in patients at risk of secondary cervical injury: a randomised controlled trial. Eur J Anaesthesiol. 32, 615-623 (2015).
- Williams, K. A., Barker, G. L., Harwood, R. J., Woodall, N. M. Combined nebulization and spray-as-you-go topical anaesthesia of the airway. Br J Anaesth. 95, 549-553 (2005).
- O'Hare, D. O., Harwood, R., Woodall, N., Barker, G. A method of administering topical anaesthesia for flexible airway endoscopy. Anaesthesia. 55, 616 (2000).
- Long, T. R., Wass, C. T. An alternative to transtracheal injection for fiberoptic intubation in awake patients: A novel noninvasive technique using a standard multiorifice epidural catheter through the bronchoscope suction port. Anaesthesiology. 101, 1253 (2004).
- Xue, F. S., et al. Spray-as-you-go airway topical anesthesia in patients with a difficult airway: a randomized, double-blind comparison of 2% and 4% lidocaine. Anesth Analg. 108, 536-543 (2009).
- Hershey, M. D., Hannenberg, A. A. Gastric distension and rupture from oxygen insufflation during fiberoptic intubation. Anesthesiology. 85, 1479-1480 (1996).
- Ho, C. M., Yin, I. W., Tsou, K. F., Chow, L. H., Tsai, S. K. Gastric rupture after awake fiberoptic intubation in a patient with laryngeal carcinoma. Br J Anaesth. 94, 856-858 (2005).
- Chapman, N. Gastric rupture and pneumoperitoneum caused by oxygen insufflation via a fibreoptic bronchoscope. Anesth Analg. 106, 1592 (2008).
- Ovassapian, A., Mesnick, P. S. Oxygen insufflation through the fiberscope to assist intubation is not recommended. Anesthesiology. 87, 183 (1997).

{kind=link}